The effect of the use of smartphone while walking on the electromyography activity of the lower extremity in young students
Article information

Abstract
The study aims to determine the effects of smartphone use on the muscle activity of the lower extremity when walking. Twenty-three healthy young students were asked to perform a 10-m walk test between normal walking without using a smartphone and walking while two-handed texting on a smartphone. The electromyography activities of the lower extremity were quantified. To quantitatively assess the cervical flexion range of smartphone users, the cervical flexion angle was measured using a digital goniometer. The study results indicated that the use of a smartphone while walking could lessen muscle activity on the tibialis anterior, gastrocnemius, rectus femoris, gluteus maximus, and gluteus medius than that of normal walking without using a smartphone. The walking speeds were reduced in walking while using a smartphone compared with normal walking without using a smartphone. The cervical flexion angle was greater when walking while using a smartphone compared to that of normal walking without using a smartphone. These results suggest that frequently using a smartphone while walking could be a potential risk for musculoskeletal problems.
INTRODUCTION
Walking has been associated with many advantages for people’s well-being and physical health (Abraham et al., 2010). Understanding individual muscle forces during walking can help to better identify several musculoskeletal injuries from gait analysis and provide a better insight on how these affect walking (Lin and Huang, 2017).
Electromyography (EMG) has been used to monitor the electrical activity in the lower limb muscles (Alghamdi and Preece, 2020). Some studies have researched how muscles contribute to support and the progression during normal gait (Anderson and Pandy, 2003; Liu et al., 2006; Neptune et al., 2001, 2004). Neptune et al. (2008) reported that the gluteus maximus, vasti, soleus, and gastrocnemius were influential for trunk support over a range of walking speeds.
Smartphones are considered a necessary part of the daily life in all age groups. An estimated 77% of the world’s population owns a smartphone, where texting emerged as a quick and cost-effective communication method (Schabrun et al., 2014). In a study conducted from 2014 to 2015, 2,367 students from the Saudi University participated. Of these 2,367 students, 27.2% admitted using their smartphones for more than 8 hr per day and 75% of them admitted using it for 4 hr a day (Alosaimi et al., 2016). Excessive smartphone use is associated with repetitive strain on joint, resulting in inflammatory changes in healthy joints (Megna et al., 2018). According to a research, 82% of the smartphone users experienced pain in the back, shoulder, neck, and hands, with greater severity associated with more time spent on their devices (Berolo et al., 2011). In cities, human behavior when walking has changed greatly: many pedestrians now use their smartphones while walking (Basch et al., 2015). Nasar and Troyer (2013) reported a 6-fold increase in the incidence of smartphone-related pedestrian injuries from 2005 to 2010. Given the increasing rate of smartphone use, it is unlikely that this trend will reverse without countermeasure. Using a smartphone while crossing a virtual street increased the time spent looking away from the road and the frequency of car crash (Byington and Schwebel, 2013). It may alter walking as a result of the increased cognitive demand placed on the working memory and the executive control during dual-task performance (Rubinstein et al., 2001).
A previous research has shown that using a smartphone while walking leads to changes in gait, characterized by decreased step length, increased step width, longer standing on each limb, and a decrease in swing time (Parr et al., 2014). In another study, researchers measured severity of the head-forward tilt posture of smartphone use and found that those using a smartphone while sitting and standing tend to put their heads down (Lee et al., 2015). The head-down posture when using smartphones contributes to the occurrence of neck musculoskeletal disorder (Berolo et al., 2011). The pain occurs in the neck and other body parts, including the wrists, hands, thumbs, and fingers (Barr et al., 2004; Gustafsson et al., 2010; Ming et al., 2006).
Recently, healthy young individuals walked with more thoracic kyphosis and lumbar lordosis when using a smartphone compared to when walking without using a smartphone. The results show that the routine use of a smartphone while walking could be a risk for low back pain and musculoskeletal disorders (Choi et al., 2021). Betsch et al. (2021) investigated that the excessive smartphone use can lead to major changes in the spinal posture, such as increased trunk inclination and thoracic kyphosis while standing and walking.
However, no study has yet quantified the EMG of the lower extremity muscles when using a smartphone while walking. To further explore the effects of smartphone use on walking, we examined and compared the EMG amplitudes of the lower extremity muscles during normal walking without using a smartphone and texting on a smartphone while walking. We hypothesized that walking while using a smartphone would change the lower extremity muscle activity compared to normal walking.
METERIALS AND METHODS
Participants
Twenty-three healthy young students (14 males, 9 females) were recruited from the university community, with the inclusion criteria of belonging to the study target. The exclusion criteria were having a history of fracture of the pelvis and the lower extremity, diseases affecting walking, and not understanding the evaluator’s commands. In our survey, it was reported that the participants spend an average of 329.13±61.92 min per day using smartphones. The subject characteristics are presented in Table 1. This study was approved by the Ethics Committee of U1 University (approval number: 2020–07). All subjects provided written informed consent.
General characteristics of the subjects (n=23)
Methods
Each participant walked flat on the ground in two different conditions: normal walking without using a smartphone and walking while conducting two-handed texting on a smartphone. The subjects were asked to text the first verse of the national anthem. After shaving, debriding, and cleaning the skin surface, electrodes were placed over the following eight right lower limb muscles: gluteus maximus and medius, biceps femoris, rectus femoris, gastrocnemius (medial and lateral parts), tibialis anterior, and soleus. With a tape, the surface electrodes were positioned longitudinally over the abdominal muscle, approximately in the direction of the muscle fibers, according to the SENIAM recommendations (Table 2) (Hermens et al., 2000). While conducting the walks, the EMG signals from the muscles were collected using a surface EMG system.

Electrode location descriptions on the muscle
Electromyography
To acquire EMG signals, the surface EMG data were recorded using a Trigno wireless EMG system (Delsys, Inc., Boston, MA, USA). Data analysis was performed using the EMGworks software package (ver. 4.0; Delsys). The sampling rate for the EMG signal was set at 2,000 Hz and the band-pass filter between 20 and 450 Hz. The raw data from the muscles were transformed into the root mean square data. A reference voluntary contraction (RVC) was used to normalize EMG data (Lehman and McGill, 1999). The mean values for the RVC were calculated from each muscle when the subjects were in a static standing for 10 sec.
10-Meter walk test
The 10-m walk test (10-MWT) is a simple assessment to measure walking ability in clinical settings, where an individual independently walked a 14-m distance. The time taken for the intermediate 10 m is measured, allowing acceleration and deceleration. It can be either tested at the preferred walking speed.
Digital goniometer
The cervical flexion angle in the sagittal plane was measured from each participant while walking and texting on a smartphone and while normal walking without using a smartphone after 10-MWT immediately. The digital goniometer axis was placed at the external auditory meatus and the stationary arm perpendicular to floor. Finally, the moving arm was placed at the base of the nostrils. In the 0 starting position for measuring the cervical flexion range of motion, the goniometer reads 90°, which should be transposed and recorded as 0°.
Statistical analysis
Statistical analyses were performed using the IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA), where the data were expressed as means±standard deviations. The differences between normal walking without using a smartphone and walking while texting on a smartphone were assessed by performing the Wilcoxon signed-rank test, considering a P-value of <0.05 as statistically significant. In all measurements in the data, the average value of the three repetitions was calculated.
RESULTS
Electromyography
For walking without using a smartphone and walking while using a smartphone, the mean normalized EMG values of the tibialis anterior were 689.07%±441.75% and 595.08%±400.86%, medial gastrocnemius 1,040.37%±1,127.66% and 888.10%± 988.52%, lateral gastrocnemius 650.72%±504.10% and 494.05%±363.58%, rectus femoris 785.53%±960.66% and 695.36%±989.98%, gluteus maximus 1,398.78%±2,730.48% and 930.33%±1,943.44%, and gluteus medius 1,201.03%± 3,745.77%, and 950.49%±3,257.50%, respectively, showing a significant difference between the two walking tasks (P<0.05). The mean normalized EMG of the biceps femoris was lesser during walking while using a smartphone (1,455.29%±2,315.15%) than that during normal walking without using a smartphone (1,906.61%±3,444.23%), having no significant differences (P> 0.05). The participants used the soleus muscles more during walking while using a smartphone (1,973.66%±7,461.34%) than during normal walking without using a smartphone (1,704.35%± 5,863.38%), showing no significant differences (P>0.05) (Table 3).
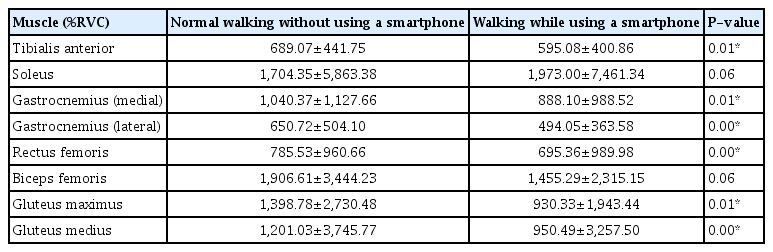
Comparison of muscle activity
10-MWT
The walking speed was slower during walking while using a smartphone (10.15±1.29 sec) than that during normal walking without using a smartphone (8.92±1.10 sec) (P<0.05) (Table 4).

Comparison of the 10-meter walk test

DISCUSSION
The study aims to determine the effects of smartphone use on the lower extremity muscle activity during walking. Our results show that the participants walked with less muscle activity in the gluteus maximus and medius, biceps femoris, rectus femoris, gastrocnemius, and tibialis anterior when using a smartphone compared to when walking without using a smartphone. Researchers found that the vasti, hamstring, gluteus maximus and medius, soleus, gastrocnemius, and dorsiflexors were the central factors of the fore-aft and vertical ground reaction force or the center of mass accelerations while walking (Liu et al., 2006; Neptune et al., 2004). Neptune et al. (2008) reported that the vertical support of the trunk was provided by the vasti, gluteus maximus, gastrocnemius, and soleus, while the forward propulsion of the trunk was provided by the rectus femoris and soleus.
Previous studies analyzed that the hip and knee extensor muscles provide much of the support in the first half of the stance phase (Kepple et al., 1997; Neptune et al., 2004; Pandy, 2001; Winter, 1980). During the early stance, the quadriceps femoris muscle slows the forward progression and affords vertical support (Liu et al., 2006, 2008; Neptune et al., 2004). The gluteus medius is considered the major hip abductor (Flack et al., 2012), with a main function of weight bearing for pelvic stability in the unilateral stance phase against the effects of gravity (Al-Hayani, 2009; Gottschalk et al., 1989). Also, it makes considerable contributions to the vertical acceleration in the single limb support (Anderson and Pandy, 2003).
In the human body, the gluteus maximus is the largest muscle (Ward et al., 2009), which arises from the back bone of the pelvis, attached to the side and back of the upper femur. Its action is hip extension, performing as the major propulsive muscle during upright walking (Lovejoy, 1988). The muscle functions to control the flexion of the trunk relative to the stance limb during walking (Anderson and Pandy, 2003). Interestingly, the human walking economy is a shorter and more dorsally projecting ischium, enabling hip extensor muscle torque production at 180° full extension of the hip (Lewton and Scott, 2017; Stern and Susman, 1983). Because of this feature, the straight-legged gait advances walking economy compared to nonhuman apes by decreasing the muscle activity needed to support the body weight in each step (Pontzer et al., 2009; Sockol et al., 2007).
During human walking, the tibialis anterior absorbs energy across the ankle joint as the foot comes in contact with the ground, producing force during the ankle plantar flexes (Usherwood et al., 2012) and plays a major role in controlling foot position and ensuring toe clearance. It is active at the end of the stance phase and into the early swing phase, to help power the ankle dorsiflexion (Hof et al., 2002). The gastrocnemius is important in stair climbing, walking, and running and, together with the soleus, accounts for about 93% of the plantar flexion torque (Haxton, 1944). The soleus is a one-joint muscle running from the back surface of the fibula and tibia to the Achilles tendon. And its activations are during the end part of the loading response phase, working until the end of the terminal stance phase. The gastrocnemius is a two-joint muscle with two heads located from the medial and lateral condyles of the femur (Park et al., 2019). In gait cycle, the gastrocnemius is active between 10% and 60% and contributes in producing energy between 40% and 60% when the ground reaction force is directed forward and upward (Nadeau et al., 1999). Eventually, the decrease in gastrocnemius muscle activity while walking using a smartphone would cause difficulty in producing proper energy for walking.
Our study results showed that contrary to the gastrocnemius, the soleus muscle more while walking using a smartphone than in normal walking without using a smartphone, but not statistically significant. There is sufficient evidence showing that decreased medial gastrocnemius force generation would require an increase in soleus activation to maintain enough ankle joint torque (Cronin et al., 2011; Lichtwark and Wilson, 2008). In the present study, the walking speed evaluation revealed that individuals walk slower when walking while texting than normal walking. Researchers indicated that walking speed decreased when texting on a smartphone, which they explained to be caused by the cognitive distraction of a dual task (Lamberg and Muratori, 2012).
Our results showed that the cervical flexion angles were 4.27° and 30.79° for walking without using smartphone and walking while using a smartphone, respectively, with a significant difference between the two tasks. This finding was consistent with the earlier result, where the mean cervical flexion angle was 38.5° for walking while texting on a smartphone. They reported that the use of a smartphone while walking poses potential risks for neck musculoskeletal problems due to a large neck flexion (Han and Shin, 2019). The neck flexion increases the moment arm of the head with respect to the rotation axis at the cervical level, and it involves the contraction forces of the neck extensor muscles to support the head weight in the flexed neck (Straker et al., 2008). The increased neck flexion while using a smartphone can have major effects on the entire spine since it is connected in a kinematic chain of joints. Moreover, greater head motion may reduce the vestibular information. The vestibular input is essential for navigation during walking (St George and Fitzpatrick, 2011). In an earlier study, the neck flexion angle has been quantified as a potential risk factor leading to biomechanical stress at the cervical level when using a tablet (Douglas and Gallagher, 2017; Young et al., 2012).
A recent study found that healthy young individuals walked with more thoracic kyphosis and lumbar lordosis when using a smartphone compared to when walking without using a smartphone (Choi et al., 2021). Additionally, walking while using a smartphone may slightly increase the pelvic anterior tilting, knee hyperextension, and ankle plantar flexion, thus, rendering less muscle activity of the gluteus maximus and medius, biceps femoris, rectus femoris, gastrocnemius, and tibialis anterior compared to when walking without using a smartphone. In summary, the flexed head during walking while using a smartphone lowers the center of gravity, activates more muscles of the neck (Yoon et al., 2020) and lumbar area (Choi et al., 2021), and lessens the activation of the extensor muscle in the lower extremity. Muscle activity imposes less load to the less active muscles and greater load to more active muscles (Kouzaki and Shinohara, 2006). Consequently, the changes in muscle activity during walking associated with smartphone use may undermine functional walking in common pedestrian environments. The frequent use of a smartphone during walking could be a risk factor for musculoskeletal disorders.
There are some limitations to be noted. First, the participants of this study only walked for a short distance in a controlled laboratory space under controlled walking conditions. Second, we only evaluated young students in their 20s and not all ages. Third, the sample size of this study was too small for generalization. Future study should include enough walking distance and many people to cover various situations of smartphone use.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
The authors received no financial support for this article.