Prevalence of metabolic syndrome in the Gulf Cooperation Council countries: meta-analysis of cross-sectional studies
Article information

Abstract
Metabolic syndrome is a collection of health-related conditions that lead to serious health condition. An individual with metabolic syndrome may acquire greater risk for adult-onset complications such as cardiovascular or neurological disorders. The aim of this study was to review and provide the prevalence of metabolic syndrome in Gulf Cooperation Council countries (GCC). Literature searches were performed on PubMed, Google scholar, and Web of Science Core Collection for English-language articles along with national studies. The following search terms were used during search: “prevalence of metabolic syndrome in GCC,” “prevalence of metabolic syndrome in middle east,” “prevalence of metabolic syndrome in Arab,” and “prevalence of metabolic syndrome name of country.” Thirty-seven studies were selected for final review out of 132 studies. The weighted pooled prevalence of metabolic syndrome was 27.3% with high heterogeneity (I2=98.94%; Cochran Q-test P<0.01). The results showed comparatively high and rising rate of metabolic syndrome in the GCC area. Preventative strategy should be considered to reduce the risk of morbidity or mortality related to metabolic syndrome.
INTRODUCTION
The metabolic syndrome has been known to acquire by sedentary lifestyle and calorie rich eating habit. Various metabolic factors may lead to development of life strengthening diseases such as cardiovascular disease, type 2 diabetes, dyslipidemia, and hypertension (Ranasinghe et al., 2017). Although adult-onset diseases may solely occur without the metabolic factors, the risk for the co-occurrence has been known to increase by several folds with the existing metabolic factors (Mente et al., 2010). The most common definitions used to define metabolic syndrome were reported by the World Health Organization (WHO), European Group for Study of Insulin Resistance, National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), International Diabetes Federation (IDF), and Joint Interim Societies (JIS). The metabolic syndrome was defined by basically similar components that included terms. For example, WHO used components such as impaired fasting glucose, impaired glucose tolerance, homeostatic model assessment for insulin resistance, obesity, dyslipidemia, hypertension, waist circumference, and blood pressure as criteria. The NCEP ATP III used components such as fasting triglyceride, fasting high-density lipoprotein, fasting blood glucose as criteria for prevalence of metabolic syndrome (Huang, 2009).
The member states of the Gulf Cooperation Council (GCC) include Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the United Arab Emirates. Recently, the prevalence of the type II diabetes mellitus and related adult-onset disorders have reported to be high in the GCC countries. Several publications reported that four out of six countries of the GCC countries are among the top 10 countries with the greatest prevalence rate for adult-onset type 2 diabetes and cardiovascular diseases (Al-Lawati et al., 2008; Kamran et al., 2007; Ranasinghe et al., 2017). The rapidly increasing rate of the adult-onset chronic complications such as type 2 diabetes and cardiovascular diseases have been related to the changes in the environment and lifestyle that lead to sedentary lifestyle and consumption of food high in calorie (Malik and Razig, 2008). Despite various studies on the prevalence of metabolic syndrome in the GCC countries, the overall report on the metabolic syndrome in the GCC countries is scarce. Therefore, this report was conducted to provide the evidence-based prevalence rate of metabolic syndrome in the GCC area through meta-analysis. Providing evidence- based prevalence rate of the metabolic syndrome in the GCC area could contribute fundamental foundation for developing scientifically supportive evidence for the metabolic syndrome prevention campaign.
MATERIALS AND METHODS
This study is a systemic review prepared by the meta-analysis based on the guidelines provided by the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis protocol) (Moher et al., 2010; Shamseer et al., 2015).
Data sources and search phrases
In order to obtain evidence-based study results on the prevalence rate for the metabolic syndrome, electronic literature searches were conducted on the web-based database sites such as the PubMed database, Google Scholar, and Web of Science collection. Only the English-language research articles with the nation-wide or population-based subjects were gathered for this study. The initial data collection was conducted without filtering for time. Specific search terms or phrases were used to find the articles. The search phrases included “prevalence of metabolic syndrome in middle east,” “prevalence of metabolic syndrome in Arab,” “prevalence of metabolic syndrome,” “name of country,” and “metabolic syndrome.”
Article selection procedure
After the initial gathering procedure, the selected articles were considered for inclusion based on the following inclusion and exclusion criteria. This study used broad inclusion criteria to provide comprehensive systemic reviews of the topic.
First, the articles were considered for inclusion if the articles were original research studies and reported on the prevalence rate for the metabolic syndrome. There were no restrictions on the study type unless the articles are review articles. Cohort and cross-sectional studies were also included. Geographic regions such as urban or rural regions were not excluding criteria. The studies on specific clinical complications such as diabetes, acute coronary syndrome, ovary syndrome, or hypertension were excluded from the study. In addition, the studies that did not deal with the prevalence of metabolic syndrome as the major factor were also not included in this study. In the initial selection phase, the studies were selected based on the key terms and phrases. During the second phase, the studies were reviewed for the title and abstract for exclusion. Finally, initially selected articles were screen and reviewed based on the full text for the final exclusion and inclusion process.
Data extraction
Information on the authors, year of publication, country of origin, sample size, gender and age of the subjects, and study design (case-control, cross-sectional or prospective cohort), metabolic syndrome identification criteria, prevalence of metabolic syndrome, and adjustment variables were obtained from the selected articles. Regarding the considerable factors and expected heterogeneity.
The random-effect model was applied for the analysis of data to obtain the expected heterogeneity and the considerable factors. The Cochran Q-test was utilized to estimate the heterogeneity between the selected studies.
Data synthesis and statistical analysis
The management and edition of data, estimation of standard error, and pooled mean effect size were estimated using Comprehensive Meta-Analysis Software (CMA) ver. 2.0 (Biostat, Englewood, NJ, USA). The pooled estimate of the prevalence rates was determined by the definitions on the metabolic syndrome provided by the ATP III, IDF, WHO, and JIS. Finally, the weighted average prevalence rates with 95% confidence interval (CI) for the selected studies were obtained by calculating the fixed effects and random effects of the meta-analysis.
RESULTS
One hundred thirty-two articles were retrieved on the prevalence or metabolic syndrome in the GCC countries through extensive search process online. After through inclusion and exclusion procedures, duplications and irrelevant articles were excluded. After reviewing the title and abstracts, 56 articles were selected for full-text screening. After the full article reviewing, seven articles were excluded due to chronic diseases, three articles were excluded since they were conducted on the subjects that were not of the GCC countries, and five were excluded for being review articles. Therefore, among 132 articles, 37 articles were selected as the final articles for the systematic review. The selection processes for the articles are shown in Fig. 1.

PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis protocol) diagram for the systematic review of the metabolic syndrome prevalence rates in the Gulf Cooperation Council counties population.
Within 37 articles, 53 different studies were identified and included for the review. Among 53 studies, 19 were published before the year 2009 and 35 were published in the year 2010 or later. Different criteria were used to diagnose metabolic syndrome in the selected studies. Fifteen studies used the criteria proposed by the NCEP ATP III for diagnosing the metabolic syndrome. Eight studies used the criteria by the IDF and 13 studies used the criteria by both NCEP ATP III and IDF. One study used the criteria by NCEP ATP III and WHO and another study used the criteria by NCEP ATP III, IDF, and JIS (Table 1). The metabolic syndrome prevalence rate is also shown as a forest plot for in Fig. 2.

Characteristics of the reviewed studies

Forest plot for the metabolic syndrome prevalence rate of Gulf Cooperation Council counties.
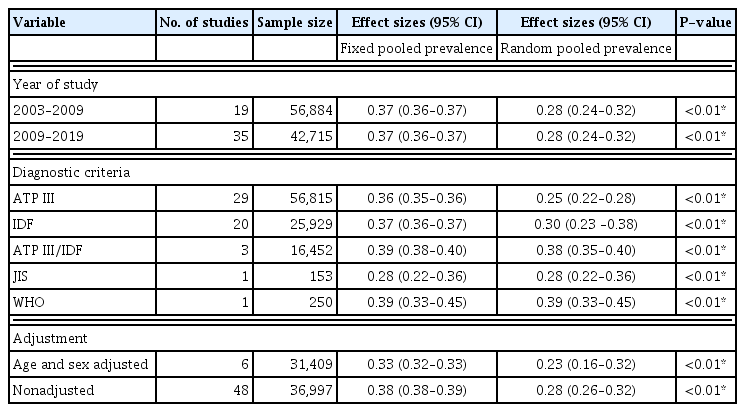
Tables 2 and 3 show the pooled estimates for the prevalence rates of the metabolic syndrome in each country and the overall pooled estimated, respectively. The prevalence rates of the metabolic syndrome in Oman was 0.25 (95% CI, 0.19–0.31), UAE was 0.39 (95% CI, 0.34–0.42), Saudi was 0.28 (95% CI, 0.24–0.33), Kuwait was 0.22 (95% CI, 0.17–0.27), and Qatar was 0.26 (95% CI, 0.18–0.37). Moreover, the pooled prevalence rates of the metabolic syndrome were estimated for the subgroups of studies (Table 4). The random pooled samples of the studies reported before 2009 and after 2010 showed the metabolic syndrome prevalence rates of 0.28 (95% CI, 0.24–0.32) and 0.27 (95% CI, 0.23–0.32), respectively.

Pooled estimations of the metabolic syndrome prevalence rate by country

Overall pooled estimation of the metabolic syndrome prevalence rate
Summary of the main results of the reviewed articles
Twenty-nine studies used the ATP III definition and the prevalence rate in the random pooled estimate was 0.25 (95% CI, 0.22–0.28). Ninety studies used the IDF definition and prevalence rate in the random pooled estimate was 0.28 (95% CI, 0.21–0.36). Three studies used both the ATP III and IDF and their prevalence rate in the random pooled estimate was 0.38 (95% CI, 0.35–0.40). One study used the JIS definition and its prevalence rate in the random pooled estimate was 0.28 (95% CI, 0.22–0.36). Finally, the last one study used the WHO definition and the prevalence rate in the random pooled estimate was 0.39 (95% CI, 0.39–0.45).
Regarding the effects of the adjustment on the random pooled estimates, six adjusted studies showed pooled for prevalence rate by the random effect of 0.28 (95% CI, 0.16–0.32). Forty-seven nonadjusted studies showed pooled prevalence by the random effect of 0.28 (95% CI, 0.25–0.31).
DISCUSSION
This study was conducted to observe the prevalence rate of metabolic syndrome in the GCC countries. In this meta-analysis review, 54 studies and 99,599 subjects were analyzed for the prevalence of metabolic syndrome. Overall, the pooled estimate of the metabolic syndrome prevalence rate in GCC was 0.28 (95% CI, 0.25–0.31). Such metabolic syndrome prevalence rate in the GCC region was greater than that of the other regions such as Latin American, Europe, Africa, and Asia. That is, the observed prevalence rate of the metabolic syndrome in the GCC countries such as was observably higher than other countries worldwide. For example, a systematic review of the countries in the Latin America region showed the metabolic syndrome prevalence rate of 24.9% with the ATP III’s metabolic syndrome definition (Márquez-Sandoval et al., 2011). A combined prospective cohort study on the prevalence rate of the metabolic syndrome reported of 15.0% in Europe with the WHO’s metabolic syndrome definition (Hu et al., 2004).
The prevalence rates of metabolic syndrome in the Sub-Saharan African regions range from 0% to 7.3% (Fezeu et al., 2007). A systematic review that reported the prevalence rates in the Asia-pacific region was 11.9% and 49.0% according to the definitions by ATP III and modified ATP III, respectively (Ranasinghe et al., 2017). On the other hand, the prevalence rates reported by the national survey in the United States were 35% and 39% according to the definitions by the ATP III and IDF, respectively (Ford, 2005). Therefore, the prevalence rate for the metabolic syndrome was high in comparison to some of the regions such as Africa or Asia while still lower than the regions such as the United States.
Over the past few decades, many of the GCC countries have experienced rapid wealth and corresponding urbanization. Such changes have led to a sedentary lifestyle by the general population due to rapid increase in the usage of motored vehicles for commuting. In addition, the working environment and facilities have changed to promote reduction in physical activity. The dietary patterns also changed in association with the environmental changes to promote inactivity and corresponding adult-onset diseases (Alzeidan et al., 2018). Conditions such as the infrastructure of the urban areas with scarce sidewalks or parks, hot arid climate, and conservative social culture restrict physical activity in the Gulf region (Alzeidan et al., 2018).
Although a vast amount of databases and articles were reviewed with detailed inclusion and exclusion criteria for the final selection limitations exist. Since a significant amount of regional reports were prepared in the native language, non-English articles could not be included in this study. The local studies that represent the regional information may provide more detailed input on the prevalence rate.
However, this is the first meta-analysis report on the prevalence ate of the metabolic syndrome in the GCC countries to our knowledge. This report may provide supportive information to prepare for the measures to intervene to prevent and control the onset of metabolic syndrome in the GCC region. It may assist to manage the morbidity and mortality rate related to adult-onset complications.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.