The effects of low-pressure hyperbaric oxygen treatment before and after maximal exercise on lactate concentration, heart rate recovery, and antioxidant capacity
Article information

Abstract
The purpose of this study was to investigate the effects of low-pressure hyperbaric oxygen (HBO) treatment before and after maximal exercise on lactate concentration and heart rate and antioxidant capacity. Ten healthy male college students were recruited from amateur soccer players. Subjects were performed a maximal exercise 3 times at intervals of at least 7 days according to the treatment method (control, pretreatment, posttreatment). Lactate concentration, heart rate, and antioxidant capacity were measured before, post, and after recovery 30 min of maximal exercise. The lactate concentration and heart rate of recovery 30 min was significantly lower in the low-pressure HBO treated group after the maximal exercise compared with the control group and the low-pressure HBO treated group before maximal exercise, and it could affect the removal of the fatigue substance caused by the maximal exercise. These results suggest that the low-pressure HBO treatment which is a new possibility for recovery of peripheral fatigue.
INTRODUCTION
Fatigue refers to the inability to develop muscle strength and the power required for muscle contraction. Rapid removal of fatigue helps improve performance and exercise performance (Costill and Hargreaves, 1992). Lactate accumulation causes fatigue, refers to the inhibition of muscle contraction by the accumulation of various metabolites such as lactate, hydrogen ion, inorganic phosphoric acid, and ammonia. The production and accumulation of lactate in the body causes acidosis by decreasing the pH, and it prevents oxidation of mitochondria and activation of enzyme (Robergs et al., 2004). In addition, lactate increases the protein binding of calcium ions in myoplasmic reticulum to negatively affect muscle contraction (Westerblad et al., 2002).
In humans, oxygen is used to produce energy and metabolism is inevitably incomplete during the metabolism (Gomes et al., 2012). In many studies, exercise is known to increase reactive oxygen species. Reactive oxygen species refers to all types of deoxygenation that are unstable due to the absence of a pair of electrons such as hydrogen peroxide (H2O2), hydroxyl radical (OH−), superoxide ion (O2.−) (Lambeth, 2004). Exercise causes active skeletal muscle contraction and increases reactive oxygen production (Powers and Jackson, 2008), leading to oxidative stress. Oxidative stress caused by the increase of active oxygen production causes damage to cells, resulting in various diseases such as diabetes, cardiovascular diseases and nervous system diseases, cancer caused by DNA damage, and promotion of aging (Reddy et al., 2009).
Hyperbaric oxygen (HBO) treatment is a minimal invasive treatment that inhales100% oxygen in chambers pressurized at 2.0 to 2.5 atmospheres absolute (ATA) (Löndahl, 2012). Originally, HBO therapy has been useful in many injuries with edema and ischemia, such as wound healing and compression injuries. HBO therapy increases the level of dissolved oxygen in the blood and increases the oxygen partial pressure of the peripheral tissues and is known to alleviate symptoms caused by low-pressure such as carbon monoxide poisoning, decompression sickness, and arterial embolism (Shimoda et al., 2015; Tibbles and Edelsberg, 1996). Recently, HBO therapy with a lower pressure (1.2 to 1.3 ATA) method has been used not only for medical but also for personal use (Edwards, 2010).
In this study, we investigated the effects of low-pressure HBO therapy before and after maximal exercise on lactate concentration and heart rate recovery and antioxidant capacity.
MATERIALS AND METHODS
Subjects
Ten healthy male volunteers were recruited from amateur soccer players who had no medical problems such as musculoskeletal diseases, cardiovascular diseases, and who does not take medication.
Before the experiment, all subjects were explained about the purpose and procedure of the experiment, and the experimental agreement. A total of three exercise tests were performed at 7 days intervals. The subjects were randomly divided into three groups: control group (n=10), low-pressure HBO-treated group before maximal exercise (n=10), low-pressure HBO-treated group after maximal exercise (n=10). The physical characteristics of subjects are shown in Table 1.
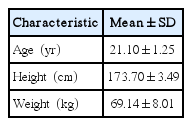
Characteristics of the participants (n=10)
Height and weight measurement
Height was measured using an extensometer (Health mate 9600A, Sewoo, Seoul, Korea) and body weight was measured using Inbody 720 (Biospace, Seoul, Korea).
Blood lactate concentration
Blood lactate concentration was obtained from the capillary blood vessels at the tip of the right hand using finger-tip method. Blood samples were taken at rest, immediately after exercise, and at 30 min of recovery. Lactate was analyzed using an automatic blood lactate analyzer (Accutrend Plus, Roche, Germany).
Antioxidant capacity
Antioxidant capacity was measured by finger-tip method using blood from the right capillary end capillary. The total antioxidant capacity of the body was determined by the BAP test (biological antioxidant potential) test. (BAP test, Diacron, Italy). Blood samples were taken at rest, immediately after exercise, and at 30 min of recovery.
Maximal exercise load test
Subjects were restricted from drinking and maintained a fasting state for 12 hr before the experiment. All experiments were conducted under the same experimental conditions and at the laboratory temperature of 23°C–24°C and relative humidity of 55%±3%. Maximal exercise was performed using a treadmill (COSMED T150, Cosmos, Germany) according to a Bruce protocol. To ascertain whether or not a maximal effort was achieved during the test, the following criteria were considered; >90% of the predicted maximum heart rate (220-age), a plateau in VO2, respiratory exchange ratio >1.15.
Low-pressure HBO treatment
Low-pressure HBO capsule was obtained from Saebo Energy (SB-153 ultimate, Seoul, Korea). Subjects were exposed to 30% oxygen at 1.3 ATA for 30 min. 1.3 ATA pressure is a pressure equivalent to 3-m depth and is the pressure that can safely provide high-pressure oxygen.
Statistical analysis
All data were expressed as the mean and standard deviation. For comparisons among the time, time×group was used mixed analysis of variance and Bonferroni post hoc test was performed with P<0.05 as an indication of statistical significance.
RESULTS
Lactate concentration
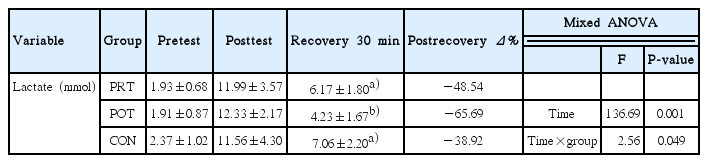
The lactate concentration was presented in Table 2. The lactate concentration in the control group was 2.37±1.02 mmol before exercise, 11.56±4.30 mmol after exercise, and 7.06±2.24 mmol after 30 min of recovery. Low-pressure HBO-treated group before maximal exercise was 1.93±0.68 mmol before exercise, 11.99± 3.57 mmol after exercise, and 6.17±1.80 mmol after 30 minutes of recovery. Low-pressure HBO-treated group after maximal exercise was 1.91±0.87 mmol before exercise, 12.33±2.17 mmol after exercise, and 4.23±1.67 mmol after 30 min of recovery. Lactate showed a significant difference in the time (F[2, 26]= 136.69, P=0.001) and time×group interaction (F[4, 54]=2.56, P=0.049). The present results showed that the lactate concentration of recovery-30 min was lower in the low-pressure HBO-treated group after maximal exercise (P=0.008).
Effect of antioxidant capacity on lactate concentration
Heart rate
The heart rate was presented in Table 3. The heart rate in the control group was 75.50±7.41 beats/min before exercise, 182.60± 7.24 beats/min after exercise, and 97.80±7.48 beats/min after 30 min of recovery. Low-pressure HBO-treated group before maximal exercise was 75.00±9.20 beats/min before exercise, 185.80±7.33 beats/min after exercise, and 96.30±4.57 beats/min after 30 min of recovery. Low-pressure HBO-treated group after maximal exercise was 74.30±7.83 beats/min before exercise, 184.70±8.00 beats/min after exercise, and 86.50±10.93 beats/min after 30 min of recovery. Heart rate showed significant difference in the time (F[2, 26]=3,045.80, P=0.001) and time×group interaction (F[2, 27]=3.92, P=0.032]. The present results showed that the heart rate of recovery-30 min was lower in the low-pressure HBO -treated group after maximal exercise (P=0.035).

Effect of low-pressure hyperbaric oxygen on heart rate
Antioxidant capacity
The antioxidant capacity was presented in Table 4. The antioxidant capacity in the control group was 2,390.20±262.67 mmol before exercise, 2,242.60±713.95 mmol after exercise, and 2,296.00± 692.88 mmol after 30 min of recovery. Low-pressure HBO-treated group before maximal exercise was 2,379.90±168.89 mmol before exercise, 2,692.50±198.59 mmol after exercise, and 2,370.10± 244.38 mmol after 30 min of recovery. Low-pressure HBO-treated group after maximal exercise was 2,307.70±269.37 mmol before exercise, 2,710.20±334.95 mmol after exercise, and 2,309.60± 156.01 mmol after 30 min of recovery. The antioxidant capacity showed no significant in the time and time×group interaction.

Effect of low-pressure hyperbaric oxygen on antioxidant capacity
DISCUSSION
HBO therapy has been used as an adjunctive therapy for diseases, and the application of HBO therapy for the treatment of sports injuries has been proposed as a therapy for primary treatment or adjunctive therapy. In addition, HBO therapy has been shown to be effective in injuries associated with bones, muscles, and ligaments (Barata et al., 2011). In this study, we investigated the effects of low-pressure HBO treatment before and after maximal exercise on lactate concentration, heart rate and antioxidant capacity.
Lactate accumulation or muscle acidosis is a major determinant of fatigue (Allen et al., 2008). Lactate removal rate is a very important factor in exercise performance, and it means inhibition of anaerobic process (Karlsson et al., 1972). In the present study, the lowest lactate showed in the treated group with low-pressure HBO after maximal exercise compared with the control group and the treated group with low-pressure HBO before maximal exercise group. The physiological response of HBO and muscle metabolism are well known. High-pressure oxygen has been shown to increase arterial pressure and reduce heart rate (Lund et al., 1999), and hyperbaric conditions have been shown to reduce serum lactate accumulation during aerobic exercise (Neubauer et al., 1999; Stellingwerff et al., 2005). Ishii et al. (2005) reported that HBO treatment showed fast recovery of lactate in the athletes. In this study, the lactate removal effect of low-pressure HBO after maximal exercise was consistent with the results of Sueblinvong et al. (2004). Heart rate recovery is known to change in response to acute changes in training load (Perini et al., 2006). Lactate concentration is known to be closely related to heart rate (Ba et al., 2009). An attenuated heart rate recovery after exercise has been shown to be predictive of fatigue (Watanabe et al., 2001). The present study showed that low-pressure HBO treatment showed significant change. However, the highest heart rate recovery showed in the treated group with low-pressure HBO after maximal exercise. These results suggest that low-pressure HBO treatment after maximal exercise alleviates the peripheral fatigue.
Oxygen is important for cellular energy systems, but excess oxygen can cause functional problems in the human body (Halliwell and Gutteridge, 1999). Early studies have shown that HBO treatment results in an increase in intracellular reactive oxygen species (Boveris and Chance, 1973; Yusa et al., 1987). However, many studies have shown an increase in antioxidant defense after exposure to high-pressure oxygen (Alcaraz-García et al., 2008; Dennog et al., 1996; Eken et al., 2005). The present results indicate that low-pressure HBO treatment before and after maximal exercise cannot mediate intracellular changes of antioxidant defense action.
Based on the present result, can be used as the new therapeutic agent for lactate control and fatigue recovery following exercise.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
This work was supported by College of Culture & Sports, Korea University Research Fund of 2018.