Neuromuscular features in sprinters with cerebral palsy: case studies based on paralympic classification
Article information

Abstract
Despite the evolution of runner performance in athletes with cerebral palsy (CP), little is known about neuromuscular parameters of sprinters from different classes, especially related to power output, muscular imbalances and asymmetry indexes in lower limbs. The aim of this study was to assess muscle power, muscular imbalance and asymmetry in sprinters with CP. Four male sprinters with CP (age, 18 to 27 years; body mass, 58.5 to 72.8 kg; height, 161.5 to 174 cm) classified as T38, T37, T36, T35 according to International Paralympic Committee functional classification, performed vertical counter movement jump and squat jump on force plate and isokinetic torque evaluations in both limbs. The concentric peak torque (PT) was measured at 60°/sec, 120°/sec and 180°/sec and PT eccentric at 60°/sec and 120°/sec. The asymmetry indexes, conventional and functional ratios were assessed. the results showed that athletes with more severe impairments (T35 and T36) showed worse performance to muscle power, more muscular imbalance and higher asymmetry in PT between limbs (> 10%). The exception was T37 athlete, who presented the better performance for all variables. it is concluded that CP athletes with more severe impairments showed lower jumping performance and torque production of knee extensors and flexors, they showed greater asymmetries between limbs. Finally, considering the results of T37 athlete, it seems that the athletic training for a longer period can reverse part of the neuromuscular impairments caused by CP.
INTRODUCTION
Cerebral palsy (CP) is defined as a nonprogressive disease that affects the development of the central nervous system, compromising the coordination of movements and posture (Sankar and Mundkur, 2005). Its prevalence around the world is 2–3.5 per 1,000 live-births (Colver et al., 2014) and the risk factors are multifactorial occurring in either prenatal, natal or postnatal care. CP is most typically associated with limitations in gross motor functioning, muscle spasticity, and cognitive impairment (Mukherjee and Gaebler-Spira, 2007). Consequently, this population has a reduction in quality of life, especially due to physical activity limitation (Rimmer et al., 2004; Ryan et al., 2017).
Sports participation is a good alternative to improve the physical and psychosocial functioning of individuals with CP (Carroll et al., 2006; Ross et al., 2016). In the Paralympic Sports program, athletes with CP are eligible to participate in several sports, being athletics (track and field) one of them. In the attempt to minimize the impact of their impairment on the outcome of competition (Tweedy and Vanlandewijck, 2011), the athletes with CP are divided into different functional sports classes: T35 (moderate diplegia and triplegia); T36 (dystonia, athetosis or ataxia); T37 (hemiplegia); and T38 (mild hypertonia, ataxia, or athetosis) (International Paralympic Committee, 2017).
Despite the evolution of runner performance in athletes with CP, little is known about neuromuscular parameters of sprinters from different classes, especially related to power output, muscular imbalances and asymmetry indexes in lower limbs. Recently, Runciman et al. (2016), verified that athletes with hemiplegia (T37 and T38) showed lower jump height with two legs in comparison with able-bodied. On the contrary, when compared nonaffected limbs, the jump height (unilateral jump) was similar between groups. In addition, the authors observed similarity in the magnitude of fatigue between athletes with CP and able-bodied post multistage shuttle run test. This behavior was observed in another study (Runciman et al., 2016) as well. Runciman et al. (2016), attribute the similarity in fatigue to the high-level training over many years of elite athletes with CP. However, these studies did not discuss differences between the studied functional sport classes.
Regarding isokinetic parameters, to the best of our knowledge, only one study assessed muscular imbalances and asymmetries in soccer players with CP (Andrade et al., 2005). The results revealed asymmetry between limbs affected and nonaffected and higher prevalence of muscular imbalance in CP group. Nevertheless, these findings are not enough to understand how much different levels of movement/posture disorders could affect neuromuscular parameters in CP athletes and consequently sport performance. Even the relationship between muscular strength and running performance remains unclear in this population. According to Beckman et al. (2016), strength could be a limiting factor for running performance, mainly for those CP athletes with more severe impairments.
In able-bodied sprinters, the imbalance among agonist/antagonist muscles has been associated with greater hamstring injury potential (Babu et al., 2016). We believe that references values to muscular imbalances and asymmetries for this population could give some directions to injury prevention and training strategies. Therefore, the aim of this study was to assess the parameters of power, muscular imbalance and asymmetry indexes in sprinters with CP from different functional sports classes. It was hypothesized that, the worse the neuromuscular parameters will be, greater the impairment of functional class.
MATERIALS AND METHODS
Participants
Participated in this study 4 athletes with CP specialists in sprint events (Table 1). They trained regularly at least 3 times per week for at least 2 hr a day. The study conformed to the standards set by the Declaration of Helsinki and was approved by the Institutional Human Research Ethics Committee of the local University. The individual anthropometric characteristic, International Paralympic Committee classification, level of competition, CP characteristics and best time to complete 100-m race are showed in Table 1.

Cerebral palsy athlete’s characteristics
Experimental design
Before assessed power and torque of lower limbs, anthropometric variables as height, body mass, and skin fold thicknesses were collected and the fat percentage was calculated based on Siri equation. Then, the athletes performed vertical counter movement jump (CMJ), squat jump (SJ), and isokinetic torque evaluations in both limbs. The concentric peak torque (PT) were measured at 60°/sec, 120°/sec, and 180°/sec and PT eccentric at 60°/sec and 120°/sec. The conventional (60°/sec, 120°/sec, and 180°/sec) and functional ratios (60°/sec and 120°/sec) were assessed. Asymmetry indexes for PT of knee extensors and flexors were also assessed for concentric contractions (60°/sec, 120°/sec, and 180°/sec) and eccentric (60°/sec and 120°/sec) contractions for both limbs. The main outcomes were jump height, peak power, PT, muscular ratios and asymmetry index.
Power of lower limbs
The analysis of muscular power of lower limbs were evaluated on force plate (Quattro Jump, model 9290AD, Kistler, Winterthur, Switzerland) during the CMJ and SJ. The frequency of acquisition was 500 Hz. CMJ: the athlete started at a static standing position with hands on the hip, and the jump was preceded by a countermovement of acceleration below the center of gravity achieved by flexing their knees to about 90°, an angle that was observed and visually controlled by the examiner. During the jump, the trunk was kept as vertical as possible, and the athlete was instructed to jump at the highest possible speed and to the highest point that they could reach. SJ: the athlete started the jump from a static position, with the knees at an angle of about 90°, the trunk as vertical as possible, and the hands on the waist. The jump was performed without any countermovement, and there was only the concentric action of the agonist muscles involved in the movement.
Before the vertical jump assessment, the participants performed a familiarization/warm-up period involving 30 sec of hopping on a trampoline, three series of 10 hops on the ground, and five submaximal countermovement vertical jumps, after familiarization athletes performed 3 attempts for CMJ and 3 attempts for SJ. The parameters were obtained as follows: (a) Jump height: calculated using the ground reaction force (GRF) double integration method, (b) peak power: greater value of the curve obtained from the multiplication of the GRF by the velocity in the concentric phase of the jump, normalized by the body mass. The stretch shortening cycle (SSC) performance gain as a percentage was calculated using the below equation: SSC performance (%)=([CMJ-SJ]/SJ)×100 (Walshe et al., 1996).
Torque measure
All participants performed a familiarization and a warm-up protocol (20 knee flexion-extension concentric submaximal repetitions at 120°/sec) using an isokinetic dynamometer (Biodex System 4 Pro, Biodex Medical Systems, Shirley, NY, USA). The participants were positioned as the manufacturer’s recommendations for evaluation of knee flexion-extension movements. Firstly, was evaluated right knee posteriorly the left knee. The same protocol was used in both limbs. After the warm-up, subjects performed 2 attempts of 5 contractions in mode concentric/concentric for quadriceps and hamstrings). In sequence, the subjects performed 2 attempts of 5 contractions in mode eccentric reactive (eccentric for hamstrings and eccentric for quadriceps muscles). For concentric contractions were used the 60°/sec, 120°/sec, and 180°/sec, and for eccentric contraction were used only 60°/sec and 120°/sec. The range of motion was 70° (30° to 100°, considering 0°=total knee extension) and 2-min rest period was respect between trials. The highest PT value obtained among the three attempts was considered the maximal torque eccentric and concentric respectively. Torque data were sampled at 100 Hz and smoothed using fifth-order, zero-phase, and recursive low-pass Butterworth filter with a cutoff frequency of 10 Hz and normalized by body mass. The conventional ratio was calculated by concentric PT of hamstrings (Hcon): concentric PT of quadriceps (Qcon) and functional ratio by eccentric PT hamstrings (Hecc): concentric PT of quadriceps (Qcon) (Aagaard et al., 1998). The data are presented as the mean±standard deviation.
RESULTS
The individual values of CMJ, SJ, and SSC are showed in Table 2. All parameters to CMJ and SJ were lower for athletes with more severe impairment. The exception was T37 athlete, who showed the higher level of training and the better time to 100 m. Besides, T36 athlete had the best use of the SSC.

Individual neuromuscular parameters assessed in CMJ and SJ
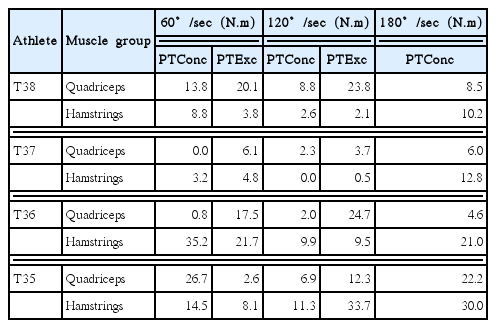
PT values were lower to T38 athlete’s left limb (affected) for all angular velocities. Differently, T37 athlete (right limb affected), showed lower PT in 60°/sec and 120°/sec in eccentric contraction and 120°/sec in concentric contraction and higher in 180°/sec concentric contraction. T36 and T35 athletes showed lower PT values in all angular velocities (Table 3).

Individual peak torque (PT) for right and left extensors/flexors of knee during concentric and eccentric contraction in different angular velocity
When analyzed the ratios, the results showed that the hamstrings in general are the weakened muscle (Table 4). The functional ratio (hamstrings eccentric: quadriceps concentric) is more affected (60°/sec and 180°/sec) (values<1). The functional ratio, by involving eccentric contractions of hamstrings, requires greater degree of coordination and showed that this muscular group produces lower PT eccentrically in both angular velocities evaluated. The conventional ratio analysis showed that higher velocity (180°/sec) seems to be most affected (values<0.60), likely due to high degree of muscular coordination involvement.
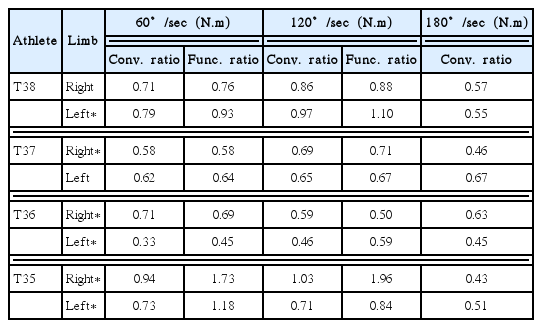
Individual conventional ratio (Hcon:Qcon) for 60°/sec, 120°/sec, and 180°/sec and functional ratio (Hecc:Qcon) for 60°/sec and 120°/sec
The athletes with hypertonia and spastic hemiplegia in one limb (T38 and T37 athletes) showed lower asymmetry index in all contraction form and angular velocities. The T37 athlete showed to be more symmetrical. On the other hand, T36 and T35 athletes presented the highest asymmetry indexes, possibly because they have more severe impairments (Table 5).
Individual values of asymmetry index (%) between lower limbs
DISCUSSION
The purpose of this study was to assess the muscle power, muscular imbalance and asymmetry in sprint runners with CP from different sport classes. The main results indicate that the athletes with more severe impairments T35 and T36 showed worse performance in muscle power, more muscular imbalance and higher asymmetry in PT between limbs. The exception was T37 athlete, who showed the best performance, which was contrary to our hypothesis. We believe that despite being an intermediate class, the high level of training of T37 athlete could explain his best performance and better neuromuscular features. This finding helps to sustain that an evidence-based classification process is crucial, because an effect of training could mask the true athlete’s sport class.
Our study showed that athlete T36 has better use (12.6%) of SSC in relation to the other athletes (T35, 8.51%; T37, 8.21%; T38, 5.15%). This finding could be explained by the fact that athlete T36 does not have spasticity. According to Lieber et al. (2004) the alterations that occur in spastic muscle (hypertonia) interfered in the better use of SSC. Considering vertical jumps, T35 and T36 athletes presented smallest performance values. These athletes had the both legs affected, different from T37 and T38 athletes who have on limb affected. The values found to CMJ (T35-19 cm, T36-21 cm, T37-46 cm, T38-29 cm and to SJ (T35-17 cm, T36-19 cm, T37-43 cm, T38-29 cm) in our study are much lower when compared with sprinters without CP (CMJ, 54.72± 5.46 cm; SJ, 51.93±4.81 cm) (Dal Pupo et al., 2012). Similarly, Yanci et al. (2016), found values to CMJ (24 cm) and SJ (20 cm) of football players with CP largely lower than that reported for players without CP.
Our findings are the first involving evaluation of isokinetic PT in sprinters with CP from different functional sports classes at different velocities. Considering PT values between limbs, we observed greater differences in T37 e T38 because they present only one limb affected. T35 e T36 showed lower PT values because the both limbs were affected. This lower performance in affected limb could be associated with central deficits include impaired central drive resulting in lower voluntary muscle activation and impaired motor unit firing rate modulation with altered firing sequencing, which could manifest as spasticity and coactivation (Moreau et al., 2009; Stackhouse et al., 2005). Beckman et al. (2017), state that strength levels are determinant for running activities among people with brain impairment, and their evaluation is encouraged as a functional classification criterion. Indeed, De Groot et al. (2012), reported moderate correlation (R2=0.34) between the PT (60°/sec) and sprint power evaluated by means of the Wingate test. In agreement, the weaker athlete (T35) and the stronger athlete (T37) in our study showed the worst and best time to 100 m, respectively.
The evaluation of muscle ratios in able-bodied sprinters is important to identify muscle imbalances and possible future injuries (Yeung et al., 2009). Such imbalances are generally related to shorter optimum angle for PT (Brockett et al., 2004), muscle fatigue (Mair et al., 1996), inadequate warm-up (Safran et al., 1998), previous injury (Gabbe et al., 2006), age (Agre, 1985), and weakness of the hamstring muscles (Croisier et al., 2002). We did not find studies in the literature that had evaluated the muscle ratios at different speeds in sprinters with CP. Andrade et al. (2005), evaluated the PT of concentric contractions at 60°/sec of soccer players with spastic hemiparesis and reported that 42% of the participants had the conventional ratio, at least of the one limb, out of normal range. Interestingly, the limb most affected by imbalances was the nonaffected by CP. The data of present study indicate a high incidence of muscular imbalances as well, both in the conventional ratio and in the functional ratio. T36 athlete showed the greatest number of imbalances. On the other hand, the T35 athlete, possibly due to the low PT values, had the lowest values of imbalances.
Athletes with CP usually show high rates of asymmetry during running (Pope and Sherrill, 1993) but it is not clear its impact on performance. Exell et al. (2012), showed that asymmetry and running performance do not have a relationship in able-bodied athletes. This could be attributed to a lower asymmetric index (<3.16%) that probably not alter the kinematic of running performance (Carpes et al., 2010). On the contrary, our data indicate that athletes who showed more severe impairments (T35 and T36) also present more asymmetric PT (>10%) and a lower running performance. Our values are similar to those reported by Andrade et al. (2005), 23%±13% between knee extensors and 24%±12% for flexors in soccer players with CP. It is interesting to mention that the authors evaluated only the 60°/sec velocity. Further studies are necessary to investigate whether such high asymmetries values are associated with the incidence of injuries and running performance. The study has limitations to be addressed. Firstly, we evaluated only four athletes. This low sample did not allow to perform a robust statistical analysis and make generalizations. Anyway, we believe that these four-case studies provided a better understating about neuromuscular features in CP sprinters. Furthermore, four sprinters with CP from different adjacent classes are very difficult to group. Secondly, despite the time spend with familiarization, mild intellectual impairments may have interfered in tests performance.
We conclude that CP athletes with more severe impairments showed lower jumping performance and torque production of knee extensors and flexors. In addition, they showed greater asymmetries between limbs. Finally, considering the results of T37 athlete, it seems that the athletic training for a longer period can reverse part of the neuromuscular impairments caused by CP.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.