Examining and comparing the health and performance indices of university undergraduate students according to year of study and gender
Article information

Abstract
This study examined and compared, based on year of study and gender, the health and performance indices of university undergraduate students. Eighty-nine students (mean±standard deviation age, 22.47±2.22 years) were randomly selected for assessment prior to second semester examination of 2015/2016 academic year. body mass index, resting metabolic rate, visceral fat, skeletal muscle mass, body fat, systolic & diastolic blood pressure, resting heart rate, upper & lower body endurance, handgrip strength, and lower back and hamstring flexibility were assessed. The students had sedentary heart rate, low skeletal muscle mass, average upper and lower body endurance, and weak handgrip strength. Significant difference existed in the visceral fat (P=0.008) between third and fourth year students. There were significant gender differences in resting metabolic rate (P=0.000), skeletal muscle mass (P=0.000), body fat (P=0.000), systolic blood pressure (P=0.001), heart rate (P=0.005) and handgrip strength (P=0.000). There are gender differences in association between health and performance indices. Dependable health education and pragmatic involvement of undergraduate university students in structured exercise programmes are recommended.
INTRODUCTION
Achievement of better health outcome for all citizenry is entrenched in the Ghana Millennium Development Goals (GMDGs) (National Development Planning Commission, 2015). Multidisciplinary and holistic approaches would be needed to accomplish a considerable progress of health and well-being of individuals in a culturally diversified nation (Reid et al., 2000) like Ghana. One of the fundamental approaches will involve the identification of indices/components that are at-risk when health is compromised (Reid et al., 2000). Body composition and cardiorespiratory functioning are some of the significantly indicted health compromised indicators in developing nations (Lee et al., 2011) due to unhealthy lifestyles. Also severe cardiovascular diseases and symptoms such as myocardial infarction (within 6 months), coronary heart disease associated with related chest pain, heart valve disorder, cardiomyopathy or other illness causing cardiac insufficiency, untreated and significantly high blood pressure (180/100 mmHg or higher), increased arrhythmias during physical effort and severe anaemia (hemoglobin 100 g/L for women and 110 g/L for men) have been well reported (Gustavo, 2010; Suni et al., 2009).
Malfunctioning or ineffectiveness in the function of the body systems as a result of the aforementioned illnesses will contribute significantly to suboptimal skill performance (Kalaja, 2012). World Health Organization (WHO) documents that as the main causes of death and disability shift to chronic and non-communicable, populations are increasingly facing modern health risks due to physical inactivity; overweight and obesity, and other diet-related factors; and tobacco and alcohol-related risks (WHO, 2009). Understanding the risks to health is key to preventing disease and enhancing motor performance effectiveness (WHO, 2009). Acquisition of knowledge is said to be essential for behaviour modification though not usually enough to make people act (Suni et al., 2009). The university students in the present study are not particularly motivated to change their personality traits because they feel relatively healthy in spite of their unhealthy behaviours like poor dietary habits, physical inactivity, long sitting hours for academic work, bad sleeping patterns, poor posture, and substance abuse. These unhealthy patterns do not match the recommendation documented in literature that every person should perform resistance training exercises for all major muscle groups-upper body, lower body, core, chest, shoulders and arms - 2 to 3 times per week (DeSimone, 2016). The lifestyle of the sampled population did not only qualify for physically inactive for not meeting regular physical activity criteria but fits into sedentary behaviour (SED) level (Hathaway and Liguori, 2017). Reported health problems, which would be inimical to investment in the education of the youth, seen in SED are hypokinetic problems, poor mental health, coronary heart disease, obesity, low back pain, osteoporosis, hypertension, diabetes, and some cancers (Biddle et al., 2010). This pretense predisposes the students to a lifestyle of hesitance to health screening despite low patronage at the recreational facilities on campus. Having realized the need for proactive measures to reduce SED and increase sedentary breaks (Hathaway and Liguori, 2017), this study examined and compared, based on year of study and sex, the health and performance indices of university undergraduate students.
MATERIALS AND METHODS
Design and subjects
A cross sectional descriptive research design was adapted for the present study. Eighty-nine students (58 male and 31 female students), mean age 22.47 (standard deviation [SD], 2.22) years were involved in the study. The participants were year one, two, three, and four students who had been in Kwame Nkrumah University of Science and Technology (KNUST), Kumasi for at least one academic semester, without known health condition, non-smokers, not under any medication or illicit drug usage and obvious disability. In 2010, KNUST launched an annual Trade and Technology (TRATECH) fair to build relevant practical projects and research works that should solve societal problems. During the 2016 TRATECH show piece of the Department of Sports and Exercise Science, consent of students were sought for assessment on the health and performance indices in this study. The 89 participants who agreed filled an informed consent form and were used for this study. A measurement laboratory room was set up in the KNUST TRATECH building by the Department of Sports and Exercise Science to accommodate measurements of the health and performance indices in this study.
Measurements
Physical
The age (years) of the participants were recorded from students’ registration file. Weight (kg) and height (m) were assessed with stadiometer (model RGZ-160, Shanghai Maney Medical Technology Co., Ltd, Shanghai, China).
Body composition
Body mass index, resting metabolism, visceral fat (VF), skeletal muscle, and body fat were assessed with the Omron Body Composition Monitor (BF511, Omron Healthcare, Hoofddorp, The Netherlands). The participants assumed recommended postures of minimal clothing; step on the main unit with dry foot on the foot electrodes and weight evenly distributed; knees and back straight, and look straight ahead. The grip electrodes were held with dry palms horizontally raised and arms extended straight at 90° angle of the body; gender, age and height were inputted into the monitor using guest mode. The unit was programmed for one-time use without resetting a personal data number. Appropriate instructions were adhered to: step on the measurement platform within about 30 sec after 0.0 was displayed; and pressed palms firmly on the grips electrodes of the display unit. Displayed value of the participants’ BMI, resting metabolism, VF, skeletal muscle and body fat were read and recorded (Omron Healthcare, 2011).
Cardiorespiratory
Systolic blood pressure (SBP), diastolic blood pressure (DBP), and resting heart rate (RHR) were measured with Omron blood pressure monitor (M10-IT, Omron Healthcare).
Performance indices
Participants underwent a 1-min push-ups (rpm) test using American College of Sports Medicine (ACSM) protocol (Pescatello, 2014). This test measures endurance of the upper body muscles (anterior deltoid, pectoralis, and triceps). Male participants were instructed to use the standard push-up protocol, whiles the female participants use the modified (bent-knee) technique. The total numbers of push-ups to exhaustion under 1 min were recorded. Wall sit test were used to measure participants’ isometric leg strength (lower body endurance). Participants were monitored to stand comfortably with feet approximately shoulder width apart, back against smooth vertical wall, and slowly slide their back down the wall to assume a position with both knees and hips at 90° angle (thighs parallel with the floor) so that feet is about 1.5 feet away from the wall. Upon assuming this position, they were instructed to hold it and timed to exhaustion using EXTECH digital stopwatch (Model 365510, FLIR Commercial Systems Inc., Exetech, Nashua, NH, USA). Handgrip dynamometer (Model 12-0241 Lite, Fabrication Enterprises Inc., White Plains, NY, USA) was used to measure the strength of the grip-squeezing muscles of the hand according to the guidelines of ACSM (Pescatello, 2014). Three trials were observed for both dominant and nondominant hands. The sum of the values obtained for both dominant and nondominant hands were divided by two and recorded as handgrip strength (kg). The acuflex I Modified sit and reach test box (Model 01285B, Novel Products, Inc., Rockton, IL, USA) was used to measure lower back and hamstring flexibility (LBHF) (Hoeger et al., 1990). Average of two trials was recorded in centimeters.
Statistical analysis
Data collected were inputted IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA) for analysis. Results of mean, standard deviation, and skewness (Table 1), One-way analysis of variance (ANOVA) with post hoc (Tables 2, 3), Independent sample t-test (Table 4) and pearson product moment correlation (PPMC) (Table 5) were used for analytical comparison. Levels of significance were set at P<0.05 and <0.01 (2-tailed).
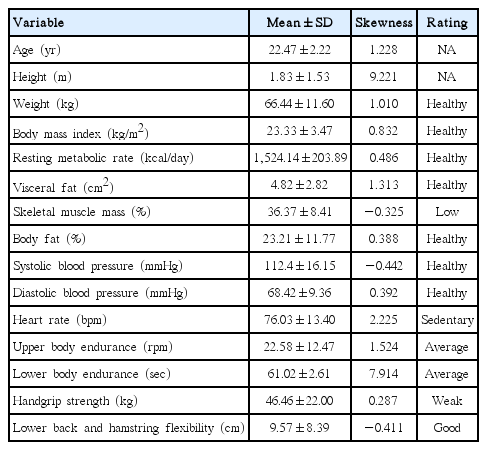
Descriptive distribution of indices (n=89)

One-way analysis of variance of indices among years in school

Scheffe post hoc analysis on visceral fat

Mean indices differences between male and female

Correlation coefficients of indices
RESULTS
The total sample population (n=89) in the study has mean age of 22.47 (SD, 2.22) years, 5 (5.6%) were first year students, second year were 14 (15.7%), those in third year were 38 (42.7%) while final year were 32 (36.0%). Male student were 58 (65.2%) and female 31 (34.8%). Information in Table 1 displays negative skewness in skeletal muscle mass, SBP and lower back and hamstring of the participants and how they stand based on rating when compared with standard normative values.
ANOVA result reveals VF as the only variable with significant difference (F[3, 89]=89.991, mean difference, 2.15625; 95% confidence interval, 0.3212–3.9913; P<0.05) according to the year of schooling with specific indicator between third and final year (P=0.014) (Tables 2, 3). T-test comparison indicates significant difference in resting metabolic rate (t=8.679, P=0.000), skeletal muscle mass (t=14.280, P=0.000), body fat (t=−10.199, P=0.000), SBP (t=3.441, P=0.001), RHR (t=−2.9033.441, P=0.005) and handgrip strength (t=8.442, P=0.000) between male and female participants (Table 4).
Results of PPMC analysis conducted among various indices with P-values were shown in Table 5. Body weight and body mass index (r=0.805, P<0.01), resting metabolic rate (r=0.808, P<0.01), VF (r=0.782, P<0.01), body fat (r=0.363, P<0.01), SBP (r=0.306, P<0.01), DBP (r=0.221, P<0.05), and handgrip strength (r=0.393, P<0.01); BMI and resting metabolic rate (r=0.466, P<0.01), VF (r=0.865, P<0.01), skeletal muscle mass (r=−0.507, P<0.01), and body fat (r=0.688, P<0.01); RMR and VF (r=0.642, P<0.01), skeletal muscle mass (r=0.389, P<0.01), SBP (r=0.427, P<0.01) and handgrip strength (r=0.652, P<0.01); VF and skeletal muscle mass (r=−0.272, P<0.05), body fat (r=0.433, P<0.01), DBP (r=0.283, P<0.01), handgrip strength (r=0.280, P<0.01), and LBHF (r=−0.220, P<0.05); SMM and body fat (r=−0.921, P<0.01), SBP (r=0.277, P<0.01), heart rate (r=−0.391, P<0.01), and handgrip strength (r=0.501, P<0.01); BF and heart rate (r=0.370, P<0.01) and handgrip strength (r=−0.405, P<0.01); SBP and DBP (r=0.351, P<0.01), heart rate (r=0.308, P<0.01), upper body endurance (r=−0.307, P<0.01) and handgrip strength (r=0.213, P<0.05); DBP and heart rate (r=0.288, P<0.01), and LBHF (r=−0.241, P<0.05).
DISCUSSION
This study examined and compared, based on year of study and gender, the health and performance indices of university undergraduate students. Findings showed that the participants are healthy based on the values of weight (Strohacker et al., 2015), BMI (Marlowe et al., 2005) resting metabolic rate (Halson, 2014), VF (Canadian Society for Exercise Physiology, 2010), body fat (Bohannon, 1997), systolic and DBP (WHO, 2009); have good LBHF (Plowman and Meredith, 2013), average upper and lower body endurance (Bohannon, 1997; Brooks, et al., 1996; Reid et al 2000), low skeletal muscle mass (Brooks et al., 1996), weak handgrip strength (Suni et al., 2009) and sedentary heart rate (Faktor, 2009) as seen in Table 1. Although the participants are reported healthy from the values of most the health components measured, Table 1 shows that their fitness level observed from performance perspective is substandard. This could be associated with the sedentary nature of their heart rates and also reflects inactive lifestyles of the participants. Physical activity and exercise participation have recorded significant correlation with improved heart rate among various population (Lee et al., 2011).
Authors hypothesized that the number of years spent in school would have reflection on the health and performance indices of university students with significant variation but this assumption is refuted based on our findings. Our finding as discovered in Tables 2 and 3 reveals no significant difference in all variables except VF across years in school. This difference may results from variation in dietary lifestyles (Elhayany et al., 2010). WHO has reported that dietary risk factors such as high blood pressure, cholesterol and obesity, coupled with insufficient physical activity, are responsible for increasing threats to the total disease burden world over (WHO, 2009).
Our findings in Table 4 shows significant differences in resting metabolic rate, skeletal muscle mass, body fat, SBP, heart rate and handgrip strength based on sex. These reiterate earlier scholarly submissions in favour of sex differences in some health and performance components of fitness (Ashwell, 2011; Egwu et al., 2012; Faktor, 2009). There are however no statistically significant differences in body mass index, VF, DBP, upper and lower body endurance as well as LBHF between males and females which supports findings in literature (Ranasinghe et al., 2013a; Reid et al., 2000). It has been argued that the rate of growth of the arm muscle tissues in males during adolescence is approximately twice that in females and that the sex difference in the growth of muscle tissue in the leg is much smaller (Busing and West, 2016). Study shows that sex-related differences in muscular development contribute to differences in physical performance because muscle strength develops in proportion to the cross-sectional area of muscle, and growth curves for strength are essentially the same (Busing and West, 2016).
Table 5 of this study shows positive correlation between body weight and body mass index, resting metabolic rate, VF, body fat, SBP, DBP, and handgrip strength. Positive correlation between body weight and body mass index, VF and body fat has been well documented (Föcker et al., 2015; Ranasinghe et al., 2013b). It has also been generally observed that resting metabolic rate is a function of fat-free mass, fat mass, dietary status and physical activity (Hudson et al., 2013). Outcome of this study reiterates the finding of a study on 145 apparently healthy individuals within age range of 14–18 years that revealed correlation between body mass and blood pressure (Ravisankar et al., 2005). Positive relationship between body weight and handgrip strength supports recent studies on the association between grip strength and blood pressure in adolescents independent of BMI (Dong et al., 2016) as well as relations between extremity muscle strength, respiratory muscle strengths and spirometric measures in a group of male nursing home residents (Bahat et al., 2014). Former study found that increased BMI is associated with enhanced blood pressure and decreased grip strength, but after adjustment for BMI, strong grip strength relates to increase in blood pressure with a concluded that strong grip strength was connected to increased adolescent blood pressure upon modification for BMI while the latter submitted that handgrip strength positively correlates with maximal inspiratory pressure and maximal expiratory pressure. The present study however presents negative significant relationship between skeletal muscle mass and BMI as well as body fat of these sample as noted in other studies (Hasan et al., 2016; Kim et al., 2014).
In this study sample, there was significant negative relationship between DBP and LBHF while the relationship between SBP and LBHF was not significant. This could reflect that BP does not serve as a predisposing agent for increase or decline in LBHF. Although LBHF is a function of muscular movement along the trunk where the heart is anatomically located, LBHF is mostly associated with hamstring muscles: semimembranous, semitendinous, and biceps femoris, located in the back of the thigh with a connection to the lower pelvis of the lower leg (Jandre Reis and Macedo, 2015). This could imply that range of motion at the trunk region of the body may not be majorly required during cardiovascular mechanism for moderate aerobic to high intensity activities of healthy living.
In conclusion, this study presents that university undergraduate students have healthy values of weight, BMI, resting metabolic rate, VF, body fat, systolic and DBP; good LBHF; average upper and lower body endurance; low skeletal muscle mass; weak handgrip strength; and sedentary heart rate. Significant difference was observed only in VF across years in school. There are variations in the differences based on gender and among measured components. Dependable health education and pragmatic involvement of undergraduate university students in structured exercise programme are recommended.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.