The effects of isometric exercise types on pain and muscle activity in patients with low back pain
Article information
Abstract
The purpose of the present study is to evaluate the effects of isometric exercise types on low back pain (LBP) patients. Isometric exercise types were mat exercise and I-Zer exercise. Subjects were divided into 3 groups: LBP control group, LBP mat exercise group, and LBP I-Zer exercise group in 23–25 aged men. Visual analogue scale (VAS) and electromyography (EMG) were used to evaluate the degree of pain and the muscle activity in LBP patients. Root mean square (RMS), median frequency (MDF), and mean frequency (MNF) were checked by EMG power spectrum analysis on longissimus thoracic (LT), iliocostalis lumborum (IL), mulitifidus (M), and rectus abdominis (RA). LBP mat exercise program and LBP I-Zer exercise program were conducted 5 sets once time, 3 times per week during 6 weeks. The two-way ANOVA with repeated measure was used to check the pain degree and muscle activity. The present results showed that muscle activity in the LBP I-Zer exercise group was increased compared to the LBP mat exercise group and LBP control group (P<0.05). LBP I-Zer exercise group and LBP mat exercise group showed increased mean frequency in LT, IL, M, and RA muscles than the LBP control group. Therefore, LBP patients performed isometric exercise may have positive effect to reduce pain degree and to increase muscle activity. Especially, LBP I-Zer exercise type showed more effectiveness in reducing pain degree and enhancing muscle activity.
INTRODUCTION
The 80% of the population suffer from low back pain (LBP) at least once or twice in a life time. LBP is known to be induced by tissue damage, muscle weakness, and psychological factor, etc (Mayer et al., 2012). Most of patients with LBP show weakened muscle strength in lumbar spine area (Solomonow et al., 2012). Increasing strength of lumbar muscle is the most important therapeutic modality for the patient with LBP. Isotonic, isokinetic, and isometric exercise has been used to improve muscle strength and endurance of muscles in lumbosacral area. Isometric exercise is safe from injury and has potent efficacy for increasing muscle strength, and it can apply to the patients with motion limitation (Kurt and Pekünlü, 2015). Mat exercise is the most used type of isometric exercise, however this exercise has difficult in controlling muscle power (Kim, 2005). The majority of isometric and resistance exercise program used the Medex device. Medex device showed improvement in pain relief and increment in muscle activity of the lumbar muscle (Hong et al., 2010). Medex device isotonic contraction was accompanied by an extension of the lumbar spine. In the present study, Medex device was to use as a device for I-Zer isometric contraction of the lumbar spine. The device also has the effect on intermittent traction with isometric contraction.
Traction therapy relaxes ligaments and muscles around the spine. And it reduces the load of the pressure within the disc. Traction techniques for patients with LBP reduce pressure on the nerve roots. Traction therapy has been used for reducing pain in the LBP (Diab and Moustafa, 2013; Wegner et al., 2013).
I-Zer exercise device is developed for isometric exercise, and this device induces intermittent movement in the spinal vertebrae by traction, and results in correction of alignment in the balance of the left and right muscles. This device has wide been used clinically, however the exact efficacy has not been proved. In this study, we compared the effects of mat exercise and I-Zer exercise device on pain level and muscle activity in the patients with LBP.
MATERIALS AND METHODS
Participants
In this study, men age 23–25 were assigned into LBP control group, LBP mat exercise group, and LBP I-Zer exercise group (n= 20 in each group). All participants were proved by doctor’s examination to perform exercise. There were no statistically meaningful differences for variables (Table 1).

Characteristics of participants (M±SD)
Experimental procedures
Pain scale test
Visual analogue scale (VAS) can be easily measured by a subjective pain score sheets, it is wildly used for the determination of the LBP. In this study, VAS is divided into vertical lines with every10 mm, from 0 point to 5 points.
Muscle activity test
Each study representative of the spectrum was used for the determination of differences in values that indicate the lumbar muscle of LBP. Values are different from normal sort of electromyography (EMG: MES9000, Apsun Inc., WA, USA), so EMG data were included in this study
EMG measures muscle activity and then skin was wiped using alcohol. And EMG data were collected using the MES 9000. The electrodes were attached both sides on LT (3 cm lateral to the first lumbar spinous process), IL (5 cm lateral to the second lumbar spinous process), MF (3 cm lateral to the fifth lumbar spinous process), and upper and lower portion in rectus abdominis (RA). The reference electrode was attached on 5th lumbar spine. For the determination of maximal voluntary isometric contraction (MVIC) in lumbar muscles, trunk was extended. For the MVIC in abdominal muscle, trunk was flexed. MVIC was determined 3 times during 5 sec with 2 min interval (MES 900 manual).
Lumbosacral isometric exercise program
Mat exercise and I-Zer exercise (101, 4CU) was conducted 5 set once time, three times per week and continued six weeks. Lumbosacral exercise on the mat was carried out in the same movement as I-Zer. The mat exercise has 5 sec exercise time and 5 sec rest time (Table 2).

Isometric exercise program
Statistical analyses
Significant difference in EMG measurement items and VAS pain level was analyzed by two-way ANOVA with repeated measure using statistical program SPSS (Ver. 21). P<0.05 was considered as significant.
RESULTS
Changes in pain scale
VAS pain rating index was decreased by mat exercise and I-Zer exercise (Fig. 1). I-Zer exercise showed more potent effect on pain relief compared to the mat exercise (P<0.05).

The change in pain levels using VAS.
Changes in the muscle activity
Muscle activity was increased by mat exercise (P<0.05) and I-Zer exercise (P<0.05) (Table 3). I-Zer exercise showed more potent effect on muscle activation compared to the mat exercise (P< 0.05).
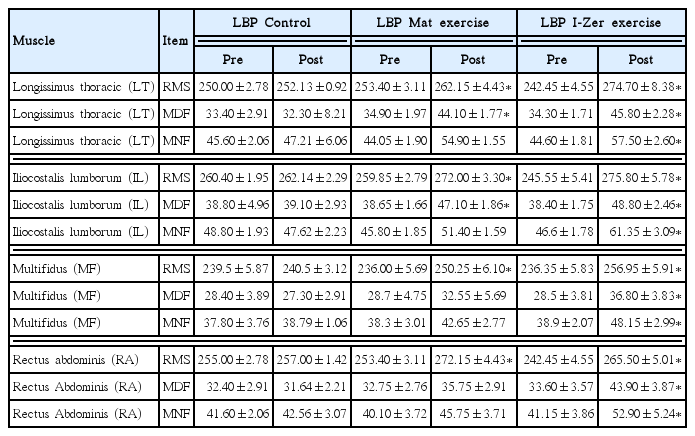
Changes in muscle activity before and after six weeks of isometric exercise (M±SD, mV)
DISCUSSION
Many studies have been made to identify the cause and treatment of LBP. The experience back pain avoids physical activity to decrease pain, which induces muscular atrophy. For the LBP persons, exercise program reducing lumbar pain has been recommended (Grgić, 2014). However, exercise therapy for pain control has not widely been used clinically. Lumbar rehabilitation exercise program increased erector spinae muscle size and reduced a pain and disability (Lee et al., 2012). Movement in lumbar rehabilitation program on the mat includes pilates, stretching, and gym, etc. Pilates on the mat enhanced muscle activity and reduced low back pain (Menacho et al., 2010). Traction therapy also reduced chronic LBP (van Middelkoop et al., 2011).
In this study, we used isometric exercise, mat exercise and I-Zer exercise, and I-Zer exercise showed more effectiveness on pain relief and muscle activation by decreasing traction and inducing relaxation. Generally, isometric training therapy (mat exercise) and exercise using a lumbosacral I-Zer device (I-Zer exercise) are designed to reduce pain by traction. Conservative treatment includes isometrics training on mat and I-Zer exercise. These exercise programs show effectiveness on reducing pain and improving function in musculoskeletal diseases (Choi et al., 2005; Taylor et al., 2007).
Increment of muscle strength and balance in lumbar spine and relief of pain could be achieved by stabilizing exercise (Han et al., 2010; Park et al., 2012), functional exercise (Shin et al., 2011), resistance exercise (Ju, 2006), and rehabilitation exercise (Lee, 2008). In the present study, disability in the activity of daily living (ADL) was decreased by isometric training on mat exercise and I-Zer exercise. These exercises showed effectiveness on LBP patients. This study will be helpful to the clinical practice. The present results could be used as the underlying method to develop more advanced techniques reducing LBP.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.