Factors influencing physical activity in older adults
Article information
Abstract
The purpose of this study was to investigate the extent to which Korean seniors report employing different motivational and social cognitive strategies related to physical activity, and to evaluate which motivational and social cognitive strategies were related to physical activity, and which motivational and social cognitive strategies differentiate between high active and low-active Korean seniors. Community-dwelling older adults (N = 187) participated in the study and completed questionnaires assessing self-reported physical activity and a range of motivational and social cognitive variables. The results showed that physical activity was predicted by quality goal-setting practices, self-efficacy, social support from family and physical activity self-regulation subscales of social support and exercise planning and scheduling. Between the groups of highly physically active and low-active participants, we observed differences in satisfaction with life, self-efficacy, quality goal-setting practices, and self-regulatory strategies related to self-monitoring, goal-setting, social support and time management. In conclusion, these findings indicate that physical activity promotion efforts among Korean older adults should focus on enhancing self-efficacy, social support, and self-regulation skills.
INTRODUCTION
By 2026, people aged 65 and over will account for 20 percent of the South Korean population. These numbers indicate that South Korea (hereafter Korea) will become the most aged society among advanced economies in 2050, with nearly four out of every 10 Koreans being aged 65 or over due to low birthrates and the rapidly aging population. Korea also boasts life expectancy (LE) one year higher than the OECD average of 80 yr, raising the important question of whether people are spending these extra years of life in good health and with good quality of life. To this end, the concept of healthy life expectancy (HALE) has been proposed, estimating the equivalent years in full health that a person can expect to live on the basis of the current mortality rates and prevalence distribution of health states in the population (OECD, 2009). HALE at birth in Korea is 71 yr (female −74 yr and male −68 yr). Difference years between LE and HALE are about 10 yr.
Sufficient and regular physical activity is one of the most widely recommended health promotion strategies for managing chronic illnesses and is known to have various health benefits (Braith and Stewart, 2006; Laaksonen et al., 2005; Lam et al., 2004; Yeom et al., 2011). Over the past 30 yr, an extensive body of evidence has accumulated regarding the benefits that accrue to older adults who participate in regular physical activity. The important role of physical activity in promoting functional health, delaying or preventing non communicable disease such as osteoporosis, coronary artery disease, non-insulin-dependent diabetes mellitus and disability, and reducing mortality has been established throughout years (Christ and Ross, 2010; Ferrucci et al., 1999; Hubert et al., 2002; Jonker et al., 2006; Leveille et al., 1999). In addition, physical activities decrease the risk of falling, improve sleep, enhance mood and general well-being, and improve blood pressure and decrease relative abdominal fat (Alessi et al., 1999; Resnick, 2001).
In spite of the established benefits of physical activity, physical activity participation remains insufficient. Approximately 28–34% of adults aged 65–74 yr and 35–44% of seniors aged 75 yr or older spend no time engaging in physical activity and inactivity is more common in women than men in the United States (USDHHS, 2006). Compared to the US, participation in regular physical activity is even less common in seniors in Korea. Approximately 80% of Korean older adults aged 60–70 yr do not engaged in moderate physical activity and 90% of older adults over 71 yr of age are inactive (Korea Ministry of Health and Welfare, 2007).
Participation in physical activity in older adults is influenced by a number of variables including demographic factors such as gender, education, and marital status. For example, physical activity participation is lower among older females (Janke et al., 2006; Weiss et al., 2007) and less educated older seniors (Droomerset al., 2001; Janke et al., 2006; Weiss et al., 2007). Interestingly, active men are more likely to have an active spouse and some studies suggest that higher levels of physical activity for older married persons have been observed (Janke et al., 2006; Pettee et al., 2006).
Additionally, choices of older adults to be regularly physically active are influenced by social support from family members or friends, availability of facilities for exercise and/or recreational activities, personal determinants especially one’s motivation, self-efficacy (i.e., a belief a person has in his or her capacity to perform a course of action), and self-regulation skills (e.g., feasible goal-setting, regular tracking of physical activity) (e.g., McAuley, et al., 2007; King and King, 2010).
In the Korean context, few studies explored the reasons why older adults engage in physical activity in Korea. Studies on physical activity with seniors have mostly focused on programs, mental health including depression and anxiety, and demographic factors but do not broadly examine social cognitive factors related to older adults’ physical activity (Cha, 2009; Lee et al., 2011; You and Won, 2010). In this study, motivational and social cognitive constructs related to Korean seniors’ participation in physical activity were examined. The main objectives were to examine 1) the extent to which Korean seniors report employing different motivational and social cognitive strategies; 2) which motivational and social cognitive strategies were related to physical activity; and 3) which motivational and social cognitive strategies differentiate between high- active and low-active Korean seniors.
MATERIALS AND METHODS
Subjects
Community-dwelling older adults (N=199) partook in a survey assessing self-reported physical activity and a range of motivational and social cognitive variables. One hundred eighty seven older adults provided sufficient data (Rangeage=57–96 yr; Meanage= 71.62±5.894 yr) to be included in the analysis after listwise deletion for missing and unreliable values. The respondents lived in a metropolitan area and a medium sized city. Researchers contacted the participants through institutions frequented by older adults such as senior centers offering various social and educational activities for seniors. Most of the participants were women (70.1%), married (71.1%), had above average education (31.6% finished high school, 30% finished undergraduate and graduate school), and more than half of the participants (52.4%) reported that they did not have any healthy problems.
Methods
Several questionnaires were used to acquire self-reported estimates of physical activity and assess the participants’ motivation to physical activity represented by a mixture of self-regulatory constructs, perceived self-efficacy and perceived social support. The Lifestyle Physical Activity Self-Efficacy Scale (LSE) (Elavsky, McAuley, 2007) and Barriers Self-Efficacy Scale (BASE) (McAuley, 1993) were used to assess the level of confidence that one can perform sufficient physical activity as part of one’s lifestyle during the following six months and in the face of barriers, respectively. The Exercise Planning and Scheduling Scale (EPS) and Exercise Goal-Setting Scale (EGS) (Rovniak et al., 2002) were used to assess strategies such as planning and goal setting. The Physical activity Self-Regulation (PASR) measured a range of motivational constructs related to self-regulation (Umstattd et al., 2009) and the Social Support for Exercise (SSE) (Sallis et al., 1987) scale was used to capture perceived social support in physical activity from friends (including acquaintances and co-workers) and family (referring to anyone living in the household). Physical Activity Survey for the Elderly (PASE) (Washburn et al., 1993) was used to measure physical activity in older adults. The 12-Item Short-Form Health Survey (SF-12) was used to assess physical and mental health status (Ware et al., 1996) and the Satisfaction with Life Scale (SWLS) measured global quality of life (i.e., satisfaction with the respondent’s life as a whole; Diener et al., 1985).
All used questionnaires were translated from English for the purpose of the study and supplemented by back-translation to ensure the accuracy of the translation; they also showed acceptable internal consistency (Cronbach’s alpha=0.61–0.97) in the study. Most scales were 5 point Likert scales with 1 representing “never” and 5 representing “very often.” The self efficacy scales (LSE and BASE) were 100 points scales with responses indicated in 10-point increments.
Analysis
All data obtained from the measures were processed by the SPSS (ver. 21.0) statistical software. To address goal 1, descriptive statistics were generated to describe the relative use of a variety of motivational strategies in the participants. To address goal 2, bivariate correlations were computed between the motivational constructs and self-reported measures of physical activity and conducted multiple regression analysis was used to evaluate unique contribution of each factor to explained variance in physical activity. To address goal 3, we compared motivation strategies implemented by the physically high active and physically low-active groups using independent two-sample t-test. We used 150min of moderate and/or 75 min of vigorous activity per week to divide the sample into highly physically active/low-active. That is, if a person did 150 min of moderate PA or more they would be considered highly active. If they did 75 min of vigorous they would be considered active (even if they did not report 150 of moderate).
RESULTS
As can be seen in Table 1, older adults in this study strongly believed that they would be able to participate in regular physical activity (5 or more days per week for at least 30+ minutes of accumulated activities per day in the future) during the next six months (for an average LSE score of 74%). Additionally, they did believe that they would continue sufficient physical activity when they encountered diverse barriers (for an average BASE score of 73%).

Motivational strategies for physical activity (Descriptive statistics)
Participants mostly reported that they did set exercise goals (they scored high on the PASR subscale “Goal-setting”) and it was consistent with the quality of the goal setting practices such as setting both short term and long term exercise goals or analyzing the progress towards goals on the EGS scale. According to the scores on PASR “Social support” subscale, respondents in the study only rarely sought social support. They also perceived receiving low levels of support from family and friends, scoring on average 2.6 on the 5-point SSE scales.
As reflected in PASR “Reinforcement” subscale, the most prevalent motivational strategy in our samples was reinforcement seeking, such as focusing on positive emotions or health benefits of exercise. Also commonly used strategies were time management for example, reserving specific times for physical activity) and self-monitoring (i.e. participants focused on things that helped them to be active).
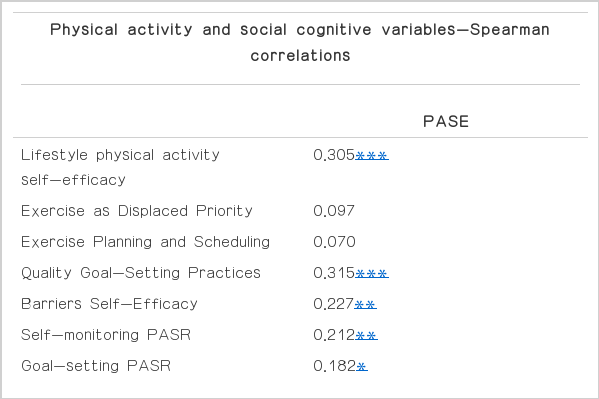
The total PASE scores were moderately correlated with a number of the motivational and social cognitive variables (Table 2), except for scores on the exercise displayed priority, exercise planning and scheduling, reinforcement, social support from family and friends, physical health and mental health scales.
Motivational and social cognitive influences on physical activity
Next, we conducted multiple regression analysis regressing separately each of the physical activity scores on the motivational and social cognitive variables. The regression coefficients and unique contributions of all variables to variance in physical activity are presented in Table 3. As can be seen, physical activity was predicted by Quality Goal-Setting Practices (β=0.321, P<0.001), Lifestyle physical activity self-efficacy (β=0.254, P<0.001), Social support exercise-family (β=−0.220, P<0.01), and physical activity self-regulation (PASR) subscales of Social support (β=0.197, P<0.01) and Exercise Planning and Scheduling (β=−0.187, P< 0.05). Overall, the motivational and social cognitive variables predicted significantly PASE score (F=10.075, P=0.000; explaining 21.8% of variance in PASE).

Motivational and social cognitive influences on physical activity
Between the groups of highly physically active and low-active participants (Table 4), we observed differences in Lifestyle physical activity self-efficacy (t=−2.959, P<0.01), Quality Goal-Setting Practices (t=−3.817, P<0.001), PASR subscales of Self-monitoring (t=−2.369, P<0.05), Goal-setting (t=−2.575, P<0.05), Social support (t=−2.827, P<0.01), Reinforcement (t=−1.180, P< 0.05), Time management (t=−2.200, P<0.05), Satisfaction of life (t=−2.485, P<0.05). Highly active older adults had significantly stronger beliefs that they would be able to maintain sufficient physical activity during the next six months. In addition, highly active participants did set exercise goals, monitored their physical activity more and participated more in physical activity when they received advises from exercise and/or health professionals. On the other hand, the high-active and low-active did not significantly differ in their scores on the EPS subscale of giving priority to exercise and planning and scheduling for exercise, BASE, PASR sub-scales of relapse prevention, and SSE. In both groups, barriers self efficacy scores were rated quite highly meaning that they would be able to participate in physical activity when they face various environmental, social and motivational obstacles. It possibly indicated that both high-active and low-active participants recognized the importance of participating in physical activity. In contrast, both group scored low on the social support especially from family indicating that the participants’ approach to physical activity was predominantly individualistic, although the high-active group perceived more support from friends rather than family.

Comparison of physically high-active and low-active older adults
DISCUSSION
Despite the increasing need for physical activity promotion efforts targeted at seniors, very little is known about motivations of Korean older adults to participate in physical activity. The aim of this study was to examine which motivational and social cognitive strategies were used by Korean older adults, which were related to their physical activity; and which differentiated between high and low active older adults.
The results showed that lifestyle physical activity self-efficacy and quality goal-setting practices were important motivational factors related to physical activity in our participants and consistent with other literature supporting the importance of these constructs. Self-efficacy is an important determinant of physical activity participation in older adults (Choi, 2004) and has predicted the maintenance of physical activity in seniors for up to 5 yr (McAuley et al., 2003, 2011). Additionally, Elavsky (2005) showed that self-efficacy often mediates that relationship between physical activity and satisfaction with life or measures of health-related quality of life in seniors. It indicates that self-efficacy plays a significant role between physical activity and some of its outcomes.
Interestingly, the participants in the study did not seem to consider physical activity as the first priority in their everyday lives. However, older adults in our study claimed that they set their own exercise goals and tried to achieve them. We found that a significant difference between high- and low-active group in this variable. This suggest that highly active Korean older adults seem to employ self-selected goal setting strategies for example setting multiple goals, monitoring the progress toward goals, setting short-and long term goals, and analyzing their goals. Using self-selected goals rather than assigned ones is associated with greater dedication and often is more valued by the individual (Hall et al., 2010; Locke and Latham, 2002).
In general we observed a weak relationship between self- regulation strategies except social support and physical activity. On the other hand, we found significant differences between high- and low- active group in some of the self-regulation strategies including self-monitoring, goal-setting, social support, reinforcement, and time management. It is possible those self-regulation strategies may be indirectly associated with physical activity or that Korean older adults participate more in lifestyle (habitual) physical activity as opposed to planful or structured physical activity that may benefit from self-regulation more directly. Mudrak et al. (2012) observed a similar set of relationship in Czech older adults. Whereas there was a week relationship between physical activity and self-regulation strategies, self-monitoring and relapse prevention significantly differentiated between active and inactive older adults. These results suggest that the effectiveness of motivational strategies such as self-regulation may vary depending on the position that physical activity occupies in older adults’ lives, which is partly culturally dependent. In Korea, not many studies have conducted the relationship between the self-regulatory skills such as realistic goal-setting, self-monitoring and physical activity among older adults even though those strategies are an important influence of behavior changes. Future researches should examine how the self-regulatory strategies play a role on behavior changes related to physical activity in the older adult population.
A number of studies demonstrated that the importance of social support to exercise behavior for older adults. Orsega-Smith et al. (2007) suggested that social support is an active and cost-effective approach to increase physical activity, and can be offered at an individual level by family, friends, or others who provide encouragement to strengthen an individual’s motives to be physically active. Indeed, social support has been shown to be an important predictor of exercise adherence among older adults (Oka et al., 1995) and to be among the most influential forces for older women to participate in active types of activities (O’Brien Cousins, 1995). In this study, the most useful form of social support appeared to stem from others such as participating in a program with friends, receiving advices from health professionals and getting demonstrations from exercise experts as opposed to from family members. The high-active group reported more support from friends and others as compared to family, a finding that is consistend with other studies suggesting that social support provided by friends rather than family domain of perceived physical ability was significantly related to leisure time physical activity (Orsega-Smith et al., 2007). More studies are needed to explore the most useful sources of social support in older adults to determine the most effective ways in which social support could be enhanced in this population.
The ambiguous role of social support from family may be indirectly related to other social phenomena such as marital status. Crespo et al. (2000) found that currently or formerly married men were more likely to be more physically active than never-married men, whereas physical activity participation did not seem to vary by marital status for women. In this study most of the participants were women (70.1%) and married (71.1%). It seems that Korean older adults, women especially, may not be receiving enough support regarding physical activity from anyone living in the household. This effect may be more pronounced for individuals who experience a divorce in later live. A study (Kim, 2009) indicated that total divorce rate has decreased in Korea but a divorce rate among older adults 65 yr and older has been increasing steadily posing additional challenges for older adults’ social support.
Further studies should be systematically conducted about different types of social support in influencing physical activity behaviors and which resources are important elements of promoting physical activity for older adults. And a variety of types of social support can be created or enhanced via social network and policy interventions to promote physical activity for seniors. Even though, self-report measures of physical activity characterize a convenient and realistic approach, and all measures used in the study have been validated for use in seniors, it may be influenced by recall bias and social desirability and differ from other objective measures for example pedometers or accelerometers. The results from this study provide a more powerful and sustainable influence on physical activity among older adults.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The study was supported by 2012 faculty research fund by the Korea National Sport University.