The effect of convalescent meridian acupressure after exercise on stress hormones and lactic acid concentration changes
Article information
Abstract
Meridian acupressure has been used as the one way recovering body conditions. The purpose of this study was to investigate whether meridian acupressure is effective on removing cortisol, norepinephrine, epinephrine, and lactic acid in blood following exercise. The subjects were 12 healthy male college students and data were processed using SPSS 12.0 statistical program and the results were calculated by setting the significance level at P< 0.05. First, there was a significant difference between exercise recovery group except for stability group and acupressure recovery group in convalescent cortisol concentration changes after exercise (P= 0.001). And acupressure recovery group showed a significant difference compared with two groups (P= 0.001). Second, exercise recovery group showed nonsignificant difference in convalescent norepinephrine concentration changes but meridian acupressure recovery group showed a significant difference (P= 0.001). There was a significance difference in the groups rather than exercise recovery group and rest recovery group (P= 0.001). Third, exercise recovery group and acupressure recovery group showed a significant difference in convalescent epinephrine concentration changes after exercise (P= 0.001). However, rest recovery group showed nonsignificant difference. In addition, three groups showed nonsignificant difference in the groups. However, it showed in order of acupressure= exercise> rest recovery. Fourth, three groups showed a significant difference in convalescent lactic acid concentration changes after exercise (P = 0.001). And it showed in order of acupressure= exercise> rest recovery after recovery treatment in the groups (P= 0.001).
INTRODUCTION
Many people try to keep their health conditions by exercise, and after exercise they take the rest through several methods. Rest is one of the important methods for the improving health status. Stress occurring during exercise induces many physiological changes including cognition. Exercise-induced physiological changes appear through nervous system and these changes can be detected by heart rate monitoring and hormone assay (Eun, 1997). Detection of cortisone in the urine and serum has been used to determine the severity of stress during exercise (Frank et al., 1992). Serum lactate concentration is also important indicator representing exercise intensity and fatigability. Kim et al. (1997) suggested that rapid removing of lactate facilitates recovery from fatigue and improves exercise performance. Cortisol level was increased before competition phase (Hejazi and Hosseini, 2012). Stress is physical and emotional response against environmental stimuli, and stress disturbs homeostasis that results in change of hormonal secretion. Catecholamine is a factor of exercise-induced psychosomatic stress (Baron et al., 1992).
Acupressure has been used as the useful strategy for the management of multiple symptoms in a variety of patient populations. Acupressure is effective for pain in patients with dysmenorrhea, during labor and after trauma. Acupressure is also effective in the management of dyspnea and in improving fatigue and reducing insomnia in a variety of populations (Lee and Frazier, 2011). Acupressure is well documented to reduce fatigue (Cho and Tsay, 2004; Tsay et al., 2004), and acupressure is effective in reducing cancer-related fatigue (Molassiotis et al., 2007; Zick et al., 2011). It was also reported that acupressure is an effective nonpharmacological adjunctive strategy for alleviating the development and progression of type 2 diabetes-related complications (Jin et al., 2009).
As exercise induces fatigue and acts as stress, many strategies have been applied to decrease fatigue and stress. Removing of fatigue after exercise is an important strategy for the exercise performance of athletes and for the health maintenance of general person. In the present study, the effectiveness of meridian acupressure on fatigue following exercise was investigated. For this, the effects of acupressure on the serum concentrations of corisol, norepinephrine, epinephrine, and lactate were evaluated.
MATERIALS AND METHODS
Subjects
Health male college students in Incheon participated in this experiment as the subjects. They well recognized the procedure of this study and agreed to this treatment. The physical characteristics of the subjects were presented in Table 1.

Physical characteristics of subjects

Experimental procedure
Exercise loading test was followed by Bruce protocol, exercise load applied to the subjects was treadmill running at 70% VO2 max for 15 min after treadmill walking for 2 min. One of the recovery methods was applied to the subjects during 1 session of experiment, and all of the subjects repeated three recovery methods during 3 sessions of experiment. The subjects in the acupressure recovery group received meridian acupressure on table for 30 min.
The subjects in the exercise recovery group performed pedaling at 0 kp for 30 min. The subjects in the exercise recovery group took rest on bed for 30 min. Blood sampling was performed 3 times via antecubital vein: before the exercise, after exercise, and after rest (Table 3).
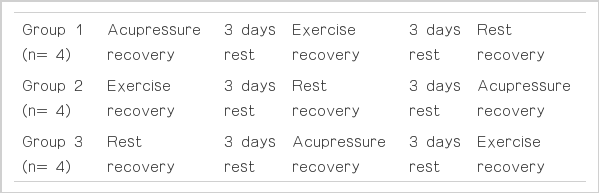
Experimental groups
Data analysis
Paired-sample t-test for the recovery types and two-way repeated ANOVA for the sampling times were used, and Duncan post-hoc was performed for the considering of statistical significance at P<0.05.
RESULTS
Cortisol concentrations according to the rest types
Serum cortisol concentration in each group after respective recovery treatment was shown in Table 4. Acupressure recovery showed most potent decreasing effect on serum cortisol concentration.

Changes of serum cortisol concentrations
Norepinephrine concentrations according to the rest types
Serum norepinephrine concentration in each group after respective recovery treatment was shown in Table 5. Acupressure recovery and exercise recovery showed more potent decreasing effect on serum norepinephrine concentration than rest recovery.
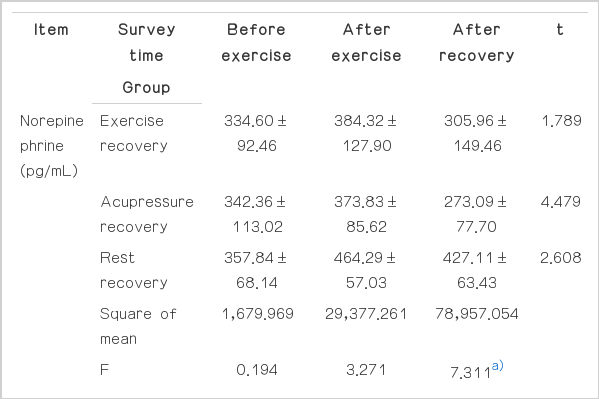
Changes of serum norepinephrine concentrations
Epinephrine concentrations according to the rest types
Serum epinephrine concentration in each group after respective recovery treatment was shown in Table 6. Acupressure recovery and exercise recovery showed more potent decreasing effect on serum epinephrine concentration than rest recovery.
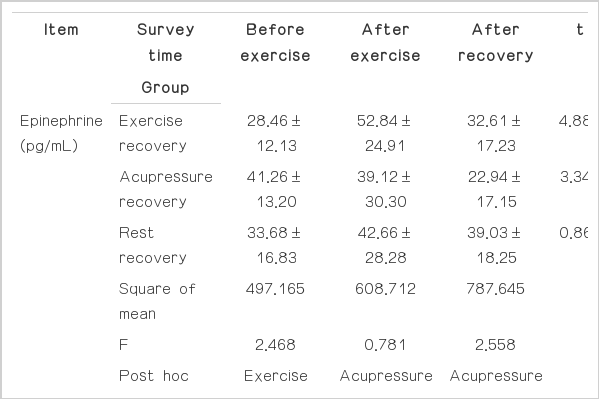
Changes of serum epinephrine concentrations
Lactate concentrations according to the rest types
Serum lactate concentration in each group after respective recovery treatment was shown in Table 7. Acupressure recovery and exercise recovery showed more potent decreasing effect on serum lactate concentration than rest recovery.
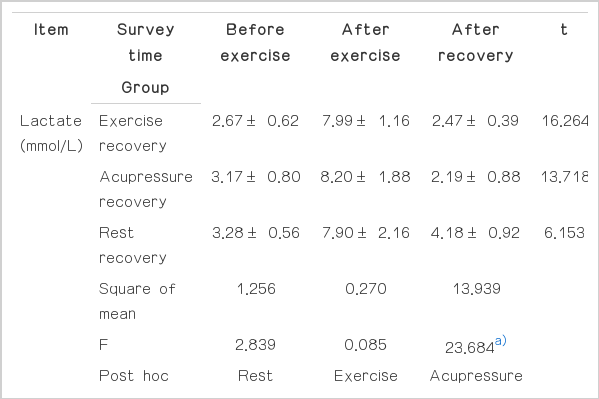
Changes of serum lactate concentrations
DISCUSSION
Although fatigue is a well-known phenomenon and the phrase “exercised until exhaustion” is commonly understood, there is no unequivocal agreement on the fundamental nature of the fatigue process (Mutch and Banister, 1983). There was a tendency for cardiac output to increase in the heat, which may have contributed to the increase in skin circulation, together with a possible further reduction in flow to other vascular beds, because muscle blood flow was not reduced (Nielsen et al., 1990). In the present study, we investigated the eliminating effects according to the recovery types on serum cortisol, norepinephrie, epinephrine, and lactate levels in the blood after exercise.
Baron et al. (1992) suggested that serum epinephrine concentration was changed by psychological stress, and exercise recovery and acupressure recovery more potently decreased exercise-induced epinephrine concentration in blood. However, norepinephrine concentration in blood was not affected by exercise recovery, meanwhile acupressure recovery suppressed exercise-induced epinephrine concentration in blood. (Baron et al., 1992). Lee and Kim (1998) reported that serum lactate level was decreased 15 min after exercise and most potent elimination effect on lactate level was observed as follows: acupressure recovery=exercise recovery>rest recovery. They showed the excellent efficacy of acupressure recovery for the lactate elimination.
Acupressure has been suggested as the ergogenic strategy through suppressing fatigue-inducing molecules in the blood. Acupressure improved the quality of sleep of elderly people and offered a nonpharmacological therapy method for sleep-disturbed elderly people (Chen et al., 1999). Patients in the acupressure had significantly lower levels of fatigue, a better sleep quality and less depressed moods compared with patients in the control group (Tsay et al., 2004). Patients in the acupressure group also showed significantly greater improvement in fatigue and depression than patients in the control group (Cho and Tsay, 2004). Acupressure is recommended as an efficacious and non-intrusive method for decreasing the agitation behaviors in patients with dementia (Yang et al., 2007). Zhang et al. (2012) suggested that acupressure exercise is feasible to be trained among postmenopausal women with knee osteoarthritis.
In the present results, we obtained following results. First, there was a significant difference between exercise recovery group except for stability group and acupressure recovery group in convalescent cortisol concentration changes after exercise. And acupressure recovery group showed a significant difference compared with two groups. Second, exercise recovery group showed nonsignificant difference in convalescent norepinephrine concentration changes but meridian acupressure recovery group showed a significant difference. There was a significance difference in the groups rather than exercise recovery group and rest recovery group. Third, exercise recovery group and acupressure recovery group showed a significant difference in convalescent epinephrine concentration changes after exercise. However, rest recovery group showed nonsignificant difference. In addition, three groups showed nonsignificant difference in the groups. However, it showed in order of acupressure=exercise>rest recovery. Fourth, three groups showed a significant difference in convalescent lactic acid concentration changes after exercise. And it showed in order of acupressure=exercise >rest recovery after recovery treatment in the groups.
The elimination effects of recovery types on fatigue-producing molecules depend on personal characteristics. The present study suggests that acupressure can be considered as the effective recovery method after exercise for the recovery from fatigue and for the enhancing of athletic performance
Acknowledgements
This research was conducted in 2011 with the support from National Research Foundation of Korea through financial resource of the government (NRF-2011-35C-G00254).
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.