The effects of abdominal draw-in maneuver and core exercise on abdominal muscle thickness and Oswestry disability index in subjects with chronic low back pain
Article information
Abstract
The purpose of this study was to effects of abdominal draw-in maneuver and core exercise with 4 weeks using the musculoskeletal ultrasonography on muscle thickness and disability in subjects with low back pain. Twenty patients with nonspecific back pain (abdominal draw-in maneuver group: n= 10, core exercise group: n= 10) were recruited in the study. Both group received exercise intervention 3 times a week for 4weeks. The test were based on muscle thickness (transversus abdominis; Tra, internal oblique; IO and external oblique; EO), disability (Oswestry disability index; ODI) measured immediately before and after intervention. The data was measured by SPSS program 12.0 version and analyzed by Paired t-test and Independent t-test. The following results were obtained. The thickness of IO, EO for both group significantly improved except for muscle thickness of Tra. The ODI were significant difference for both groups. As the results of this study, we suggest that it may be effective method to apply to increase for the thickness of Tra, EO using abdominal draw-in maneuver and thickness of IO using core exercise.
INTRODUCTION
Low back pain (LBP) is the general problem which influences the majority of adults once in their lifetime. Among those adults, most of their symptoms are naturally alleviated. However, minority undergoes LBP recurrence while the other feels constant pain (Dunn and Croft, 2004). The attack rate of LBP in lifetime is 60–80% (Waddell, 2004), and during a year, 34% (Croft et al., 1999).
Originally, LBP is associated with the technical change of the surrounding tissues of spine (Adams, 2004). The change of spinal control is caused by the hypofunction of the myotome such as transverses abdominis (Tra) (Richardson et al., 1999). Hodges and Richardson (1996, 1998) conducted the study by using EMG. They reported that the preceded posture control, preliminary to the upper limb movement activates Tra. However, in case of the LBP patients, preceded control is not working, so that its activity is being delayed. In the external oblique (EO), the larger abdominal muscle, the attack site’s activity was delayed when measured during the independent state. Also, in the internal oblique (IO), attack site’s activity showed a change during the comparative study on the non-attack site of the chronic LBP patients.
Treatments for the LBP patients were passive in the past, focusing on the pain control by taking a rest. On the other hand, active treatment is the current tendency such as lumbar trunk strengthening, for the muscle strength and stability (Bendix et al., 1996). Also, exercise therapy of the body trunk is crucial in order to improve the muscle strength and stability which is good for the deep muscle (Weinstein et al., 2006).
Abdominal drawing-in maneuver (ADIM) is the main for the strengthening of the deep muscle such as Tra, IO, and EO. ADIM is the exercise method which increases the abdominal pressure by pulling the abdominal walls to the inside that Tra and oblique abdominal are contracted. Because of the increased abdominal pressure, lumbar trunk stability training is effectively accomplished. Also, it induces the muscle contraction that excessive lordosis and tilts of the pelvis are reduced which is effective for the LBP (Kisner and Colby, 2002).
Recently, core training is on the rise as rehabilitation for the body balance. Hodges and Richardson used the term, stability and the function of the core muscle is to maintain the postural alignment. Also, maintaining dynamic postural equilibrium during the function movement as.
Tra is one of the important muscles in maintaining the stability and proprioceptive sense of the lumbar trunk (O’ Suullivan et al., 1997). This muscle controls the lumbar region’s joint because of its location and the direction of tissue. It manages the stability of the body trunk through co-contraction without a movement of joint. Core muscle system is the total component of a protective mechanism which reduces the stress that harmful forces are applying to spine during the functional movement (Barr et al., 2005).
Core stability is to maintain the inter-segmental coordination to the maximum point, and to control the body’s center of gravity from the moving basal plate. Core muscle is where all the strength and motility is arising from, it act as protecting important muscles and bones by maintaining balance whenever body moves, and muscle-skeletal structure (Brill and Couzen, 2002).
The difference between ADIM and core training is that the muscle contraction is done in an isolation state or non-isolation state. These methods have shown significance effects with LBP patients, but the comparison between the effects of these two methods are not done. Thus, what we are attempting to find in this study is the influence of ADIM and core exercise has over the thickness of Tra, EO, and IO, also over the Oswestry disability index (ODI) via musculoskeletal ultrasonic imaging. As a result, it would help LBP patients to choose the most effective exercise program.
MATERIALS AND METHODS
Experimental subject and equipments
Among W hospital patients, twenty adults were chosen as subjects of this study, and all of them were diagnosed as chronic back pain. Their sickness attacked them over six months ago. They signed to the application form before participating in the experiment which was going to proceed for four weeks. Each ten of them were divided into the group of ADIM and core training randomly. There were no statistical differences between subject’s general traits such as age, sex, height and weight (Table 1). Those who have experienced lumbar region surgery, cauda equina syndrome, progressive neurological deficit, fracture, cancer, excessive lordosis and kyphosis were excluded. In this study, 10 MHz linear probe of musculoskeletal ultrasonic diagnosis instrument, LOGIQ P5 (GE Healthcare, LA, USA) was utilized in measuring the muscle thickness. Also, physical therapists with the experience over ten years about ultrasonic measure were chosen.

Characteristics of subjects
Muscle thickness
Subjects were filmed during the Supine posture, when lordosis of the lumbar region was reduced with the help of a cushion below their knee joints. Ultrasonic head was located between the subject’s lowest ribs and iliac spine. This is where all the muscles become thicker, so that its image can be clear (Critchley and Coutts, 2002).
Oswestry disability index
Physical disability due to chronic back pain was evaluated with the self-recording survey (Fairbank et al., 1980), Oswestry disability index, which is based on the reaction and interests upon their daily life. ODI is composed of ten questions so that subjects mark grades based on their performance, 0 with no pain to 5 with the worst condition. Lower grade means that the physical disability has improved and disability index is marked as percentage dividing total grade with the answered grade. The reliability of ODI is very high which was shown in the McDowll and Newell’s (1987) study.
Exercising method
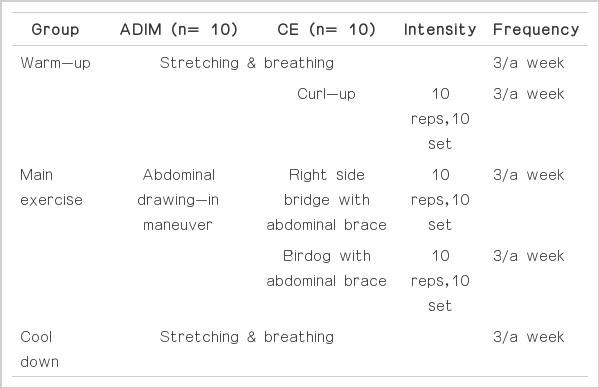
Exercise program was held three times per week, four weeks in total. Stretching and breathing exercise were carried out as a warm-up, ADIM and core training as a main program, and stretching and breathing exercise as a cooling-down. In order to make the number of times and set identical, each exercise was held ten times-ten sets. The contents and methods of the specific exercise program is the following (Table 2).
ADIM and Core exercise
Abdominal drawing-in maneuver
From the supine position to hook-lying position, with the hip joint to 40 degrees and knee joint to 80 degrees, put the cushion below knee joint and give direction to the subjects to pull the navel deeply to the lumbar region. At this time, subjects were controlled to maintain contraction while keep breathing lightly, to contract slowly, also to not move pelvis and chest while exercising (Richardson et al., 1999).
Curl-up
Subjects bend right-side knee to 90 degrees from the supine position, and put hand below the lumbar region in order to prevent spine from moving. Give directions to move head and shoulder slowly from the ground, and curl the upper limbs up with the thoracic vertebral region as an axis. Both sides of the straight muscle of abdomen showed an active response when compared with the other abdominal muscles (Kavcic et al., 2004).
Right side bridge with abdominal brace
From the reclining posture, subjects bend knees to 90 degrees, put right elbow to the ground, and hold abdominal brace. Support shoulder and knees with the body trunk without the rotation of body. One side of back extensor muscle and abdominal muscle showed an active response during this exercise (Mcgiil, 2002).
Birddog with abdominal brace
Subjects stretch left arm and right leg in a row simultaneously from the four-foot position while holding abdominal brace. Both sides of multifidus muscles, EO, and thoracic erector muscle showed an active response during this exercise (Kavcic et al, 2004).
Data analysis
SPSS 12.0 program was used in analyzing data of this study. K-S verification was used to prove the normality of the data, and a result, it was normally distributed. Paired t-test was used to compare the before and after of the exercise by using parametric test. Also, independent t-test was used to compare the change made between groups. To prove the statistical significance, significance level was set as P<0.05.
RESULTS
Change made in ODI after abdominal drawing-in maneuver and core training
The result of analyzing the change made in ODI after carrying out the abdominal drawing-in maneuver and core training for 4 weeks is the following (Table 3). In case of abdominal drawing-in maneuver, the ODI was 23.55±3.94 before the exercise and it has changed into 14.55±3.53 after which shows statistical significance. In case of core training, the ODI was 20.25±4.55 before the exercise and it has changed into 15.75±4.06 after which also shows statistical significance (P<0.05).

Pre- post comparison of muscle thickness and ODI
Change made in ODI between groups
The difference exists between the two groups, abdominal drawing-in maneuver group and core training group. First group’s ODI was 9.00±3.21, and the latter’s ODI was 4.50±3.41 that there were statistical significance between these two groups (P<0.05) (Table 4).

Between group comparison muscle thickness and ODI
Change made in the muscle thickness after carrying out abdominal drawing-in maneuver and core training
The result of analyzing the change made in the muscle thickness of Tra, EO, and IO after carrying out abdominal drawing-in maneuver and core training for four weeks is the following (Table 3).
On the comparison between the before and after of the exercise, the thickness of EO has changed 1.28±0.44 cm into 1.34±0.43 cm (P<0.05), the thickness of IO has changed 1.15±0.22 cm into 1.17±0.21 cm (P<0.05), and the thickness of Tra has changed 0.43±0.02 cm into 0.46±0.03 cm (P<0.05) that abdominal drawing-in maneuver group showed statistical significance. The thickness of EO has changed 1.12±0.34 cm into 1.15±0.34 cm (P<0.05) and the thickness of IO has changed 1.01±0.14 cm into 1.07±0.17 cm (P<0.05) that the core training group showed statistical significance as well. However, the thickness of Tra has increased 0.41±0.02 cm to 0.42±0.02 cm that there was no statistical significance (P<0.05).
Change made in the muscle thickness between groups
In terms of muscle thickness, the change made in the thickness of EO was 0.06±0.04 cm in abdominal drawing-in maneuver group, and 0.02±0.02 cm (P<0.05) in core training group. The muscle thickness of IO has changed 0.01±0.02 cm in the first group and 0.05±0.06 cm (P<0.05) in the latter group. The muscle thickness of Tra has changed 0.32±0.03 cm in the first group and 0.04±0.15 cm (P<0.05) in the latter group which showed statistical significance between groups (Table 4).
DISCUSSION
Recent studies of back pain found that the decrease of muscle mass can be the main cause of the symptom, so that the stability of the muscles around the spine and the stability of body trunk are being emphasized (Kim, 2008). Muscles around the spine contributes in stabilizing, and the imbalance of muscle induces overload to spine while moving waist (Grabiner et al., 1992). As a result, it damages the musculoskeletal system, thus pain. When the back pain occurs (Hides et al., 2001), contraction of the cross-sectional area and decrease of the function of muscles proceed rapidly to the affected sides of the lumbar region when compared with the non-affected side (Panjabi, 2003). Rather than the direct damage of spine, instability of it, such as the weakening of the deep muscles such as Tra, is the main cause of the pain since it contributes in stabilizing spine by surrounding it (Hodges, 2003). Generally, illnesses occurring to the musculoskeletal system can be treated with the preservative therapy such as exercising program, excluding the case where surgery is needed. The purpose of lumbar region strengthening exercise for the back pain increases the stability and mobility of the surrounding tissues by stabilizing the posture, also it increases the lower limb muscles strength and muscle endurance (Yoon et al., 2010).
Core training is one of the methods to stabilize the body trunk; it provides stability by resisting to the influence of gravity in order to enable humans to maintain erect posture. Core muscles include spine, abdomen, and pelvis and so on which helps extremity muscles to accomplish functional movements without the excessive stress of spine (Kisner and Colby, 2002).
Park (2012) reported that chronic LBP patient’s lumbar extensor muscle strength has improved due to 12-week core training, and also the stability has improved 4.9 percent, in terms of lumbar region’s center of gravity after the training. In the study of Lee (2009), he reported that the measured time of lumbar region muscle strength has changed 39.90 into 42.84 which show significant improvement after the 8-week core training. Teyhen (2005) found that the Tra has activated up to 109 percent after the lumbar region stabilizing training by using ultrasonic imaging. The objects were the chronic LBP patients who suffered the pain over three months.
When core training was carried out in this study, the thickness of EO has changed 1.12±0.34 cm into 1.15±0.34 cm (P<0.05) and the thickness of IO has changed 1.01±0.14 cm into 1.07± 0.17 cm that it showed statistical significance. However, the thickness of Tra has increased 0.41±0.02 cm to 0.42±0.02 cm that there was no statistical significance. This means that the core training affects the abdominal muscles and its activity and the thickness of IO/EO but it does not affects the thickness of Tra.
In case of abdominal drawing-in maneuver, Hodge et al. (2003) reported that the thickness of IO and Tra has increased whereas the thickness of EO has decreased when the objects were healthy. In the study of Beazell et al. (2006), they compared the changed ratio between healthy objects and LBP patients, that the thickness of IO and Tra has increased less among LBP patients. However, the thickness of EO has changed 1.28±0.44 cm into 1.34±0.43 cm (P<0.05), the thickness of IO has changed 1.15±0.22 cm into 1.17±0.21 cm (P<0.05) and the thickness of Tra has changed 0.43±0.02 cm into 0.46±0.03 cm (P<0.05) that it showed statistical significance in this study in case of abdominal drawing-in maneuver. In other words, the change made in IO and Tra are identical to the previous studies while the change made in Tra is not identical.
In the study of Choi (2012), the difference between the balance and walk of female olders were watched and there was no difference between two groups when body trunk stabilizing exercise and core training was carried out for four weeks. However, FRT, TUG, OLSTOE, 6MWT has improved through exercise. The study of Cho (2010) studied the influence of closed kinetic chain and core exercise over the chronic LBP youth soccer player’s muscle strength, flexibility, balance and pain. Each exercise program showed significant difference, but core training was more effective between groups. In terms of muscle thickness, EO and Tra showed more change during abdominal drawing-in maneuver while IO showed more change during core training. In terms of ODI, ADIM group showed more change. These results show that abdominal drawing-in maneuver is more effective in terms of muscle thickness of EO/Tra, and ODI. On the other hand, core training is more effective in terms of the muscle thickness of IO.
This study was conducted to find out the change made in ODI and thickness of abdominal muscles after carrying out abdominal drawing-in maneuver and core training for 4 weeks sampling 20 people hospitalized in for chronic LBP. As a result, there was significant effect on the decrease of ODI between two groups and there was also a change made in the muscle thickness of IO/EO/ and Tra when it was measured by musculoskeletal ultrasonic imaging. In conclusion, ODI and the muscle thickness of Tra/EO showed significant improvement in terms of abdominal drawing-in maneuver whereas the muscle thickness of IO showed significant improvement in terms of core training. In other words, it would be helpful to choose isolation method, abdominal drawing-in maneuver, when abdominal muscle contraction training is being carried out while non-isolation method, training would be helpful in contractive training IO and ODI. Although the reliability of musculoskeletal ultrasonic imaging and ODI were high, medicines objects are taking were not controlled, accurate education was not carried out about muscle contraction method, and the proceeding time, four weeks, was short and these would be the limitations of this study. Longer proceeding time and accurate education about exercising methods would be required in the future study.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.