INTRODUCTION
Sarcopenia is easy to cause when humans age without special care. In the process of skeletal muscle aging, muscle contractility decreases, which may increase inflammation as well as pain. Sarcopenia makes it difficult to perform even easy tasks in daily life and may aggravate a sedentary life in the elderly (Izquierdo et al., 2021). Muscle loss due to aging also can reduce the quality of life and shorten the lifespan by reducing the immunocytes function (Hadgraft et al., 2015; Shlisky et al., 2017). Previous studies have reported that sarcopenia is more serious in women than in men as the age increases (Cho et al., 2022; Jee, 2022), and it is also an opportunity to cause disorders in immunocytes (Ali et al., 2021). The decreased function of immunocyte makes it exposed to various infections, and continuous fatigue and pain increase (Booth et al., 2012). In other words, in the case of elderly women, the sarcopenia makes the immunocyte function very vulnerable.
Moderate physical activity has been reported to have a positive effect on muscle contractility as well as immunocytes function (Souza et al., 2021). Walking is the easier physical activity that everyone without specific disorders can do. A study that musculoskeletal diseases can be caused by a decrease in walking function has great implications for all humans (Song et al., 2018). In this respect, Nieman et al. (2005) reported that walking caused modest and short-lived changes in immune parameters, notably for neutrophil and natural killer (NK) cell. To our knowledge, a walking is a representative aerobic exercise that improves the contractile features of lower extremity muscles and cardiorespiratory endurance as physical activity that enables basic movement of humans. It is an exercise that is actively recommended to prevent chronic diseases (Di Loreto et al., 2005). To obtain such a preventive effect, the walking speed must be a certain level, and the effect can be obtained or maintained when it continues for more than 15 min (Hsu et al., 2006).
However, in the case of elderly person whose aging process is already continuing to some extent, it is difficult to walk without any support, and excessive walking can cause not only muscle damage, but also considerable damage to the skeletal system. That is, there are few studies suggesting how walking speeds on the muscle property of the elderly and how fast walking can improve not only muscle property, but also immunocytes. Therefore, this study aimed to investigate the changes in the lower extremity muscles when walking at various speeds was applied to the elderly women and to investigate whether changes in the immunocytes function were also caused through this change.
MATERIALS AND METHODS
Experimental design and ethical approval
A preliminary single-blinded randomized controlled trial was used to investigate how walking speed affects a muscle property of the upper legs and an immunocytes function in the elderly women. Although the subjects were elderly women who could lead an independent life and walk, informed consents were obtained from their guardians due to them being considered a vulnerable group. And, since this study had to be conducted during the coronavirus disease 2019 (COVID-19) period, the laboratory was thoroughly quarantined, and the treadmills were spaced at least 2 meters apart. This trial was approved by the ethics committee (HS22-03-01) and carried out in accordance with the Declaration of Helsinki (2013). It has also been registered in the Korean Clinical Research Information Service (KCT0007631).
Subjects
This study recruited 42 female elderly participants from 63 to 81 years of age from Seoul Seniors Tower in Seoul, Korea. To control daily activities, calorie intake, and regular exercise, the researchers took turns coresiding at the location to record all data. Utilizing G*Power (v.3.1.9.7, Heinrich-Heine-Universität, Düsseldorf, Germany), the sample size was obtained by inputting the required number of subjects in the repeated measures analysis of variance with an a priori effect size (0.40), α error probability (0.05), power (0.95), number of groups (4), and number of measurements (2) (Faul et al., 2007). It indicated that the minimum number for significance was a sample size of 32. Subjects had to meet the inclusion criteria, which consisted of not having undergone any type of treatment or having taken medication known to influence mental status and body composition. In addition, only the elderly women who had not participated in regular exercise program for more than 6 months were included. Subjects were excluded on the basis of having had any kind of psychological disorder or an impaired major organ system. If subjects who tested positive for COVID-19, or had been infected in the past, were also excluded.
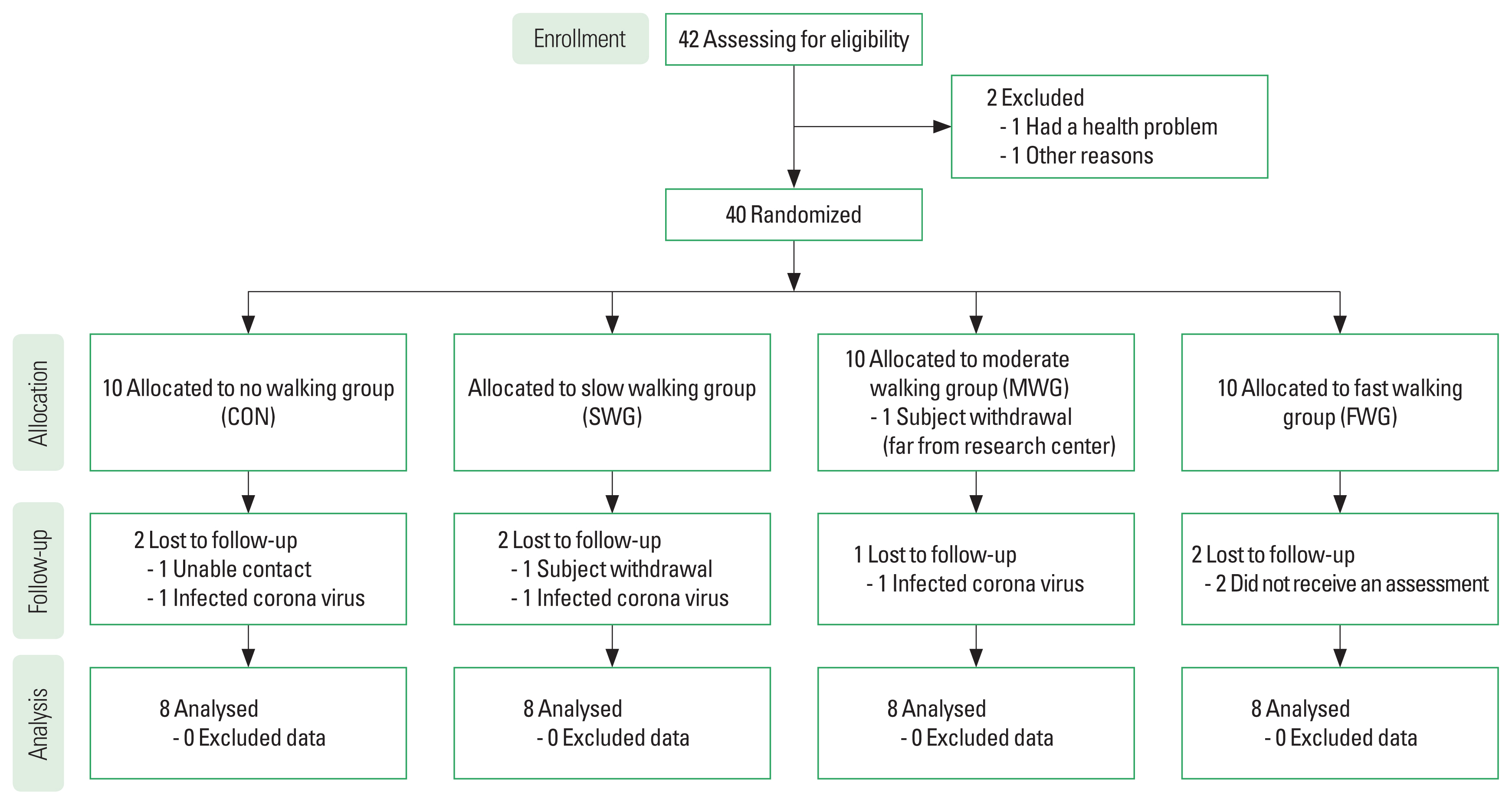
As shown in Fig. 1, 42 subjects were screened for eligibility. Before the randomization, two subjects were excluded. Forty subjects received ID numbers before being allocated to one of four groups using random number tables. The four groups consisted of the control group (CON), slow walking group (SWG), moderate walking group (MWG), and fast walking group (FWG). All subjects continued to receive standard treatment and agreed to maintain the same amount of daily physical activity and calorie intake throughout the trial. Of the 10 subjects who were allocated to the CON, a person was not able to contact, and a person was infected by coronavirus in the follow-up phase. Of the 10 subjects who were allocated to the SWG, one took a withdrawal, and a person was infected by coronavirus. Of the 10 subjects allocated to the MWG, one took a withdrawal in the allocation phase and a person was infected by coronavirus in the follow-up phase. Of the 10 subjects in the FWG, two failed to complete an assessment. In the end, this study included a total of 32 subjects. The physical characteristics of the subjects was shown in Table 1.
Measurement
Demographic questionnaire included age, disease, nutrition, and physical activity in daily life. For the muscle property, a tensiomyography (TMG) was used to gauge the static muscle features in the rectus femoris (RF) and biceps femoris (BF), and the immunocytes were identified through blood tests. The specific measurement method was as follows.
Daily nutrition calories and physical activity measures
During the session before the start of the experiment, each subject was provided a diary to record their food consumption for 12 weeks. One researcher entered the types and amounts of foods consumed by all subjects per day into CAN-Pro 5.0 (Korean Nutrition Society, Seoul, Korea) then evaluated the data weekly. The amount of physical activity was recorded each day and calculated by international physical activity questionnaire (Booth, 2000; Lee et al., 2011). Metabolic equivalent was calculated by adding the duration (min) and frequency (days) of walking (3.3×min of activity/day×days/wk), moderate-intensity activity (4.0×min of activity/day×days/wk), and vigorous-intensity activity (8.0×min of activity/day×days/wk) (Booth, 2000). The questionnaire score was used to calculate the weekly amount of physical activity.
Body composition measures
All subjects were measured for height and body composition on an Inbody 320 (Biospace Co., Ltd., Seoul, Korea) in light clothing with no metallic accessories after voiding 30 min prior. When all subjects stand on a stool with an electric current and hold the handle for about 3 min, height, weight, muscle mass, body fat mass, and basal metabolic rate are measured. This bioelectrical impedance analysis method that measured the body composition of the elderly was reported to have a very high correlation compared to the dual-energy x-ray absorptiometry method (Kim et al., 2015).
Muscle property measures
A TMG was used to assess muscle property in the RF and BF, which quantifies radial muscle belly displacement by measuring the response to a single electrical stimulus. All subjects lie in bed by a relaxed posture as the TMG test (TMG100, TMG-BMC Ltd., Ljubljana, Slovenia) was performed. The muscular contractility is enlarged due to the response to the electrical stimulus and a digital transducer measures muscle property through the acquired radial displacement pressed perpendicular to the skin over the muscles. Electrical stimulus is sent to two electrode surfaces located at proximal and distal points to the sensor. Properties of muscle contraction, including contraction time (Tc) and maximum radial displacement (Dm), are evaluated by recording the displacement-time curve (Dahmane et al., 2001; Park, 2020).
Immunocytes measures
A 10 mL of blood was assembled from subjects’ antecubital vein. Flow cytometry and antibody staining of this study were done using products of BD Bioscience (Franklin Lakes, NJ, USA). A lysed whole blood technique with eight-color staining of blood cells was used. All antibodies were titrated to determine optimal concentration. For isotype control, isotype antibodies corresponding to each antibody were used. Antibody mixtures were different in accordance with each panel. Blood samples were distributed into 12×75-nm round polypropylene bottom test tubes and stained with antibody mixtures for 30 min in the dark room. Red blood cells were lysed by adding 1 mL of FACS Lysing solution into each tube for 20 min. Cells were washed 2 times with 1×phosphate buffered saline by centrifugation at 1,500 rpm for 5 min and then resuspended in 200 μL of phosphate buffered saline. After washing, the rest cells were permeabilized by adding 500 μL of Perm/Wash Buffer for 5 min and then centrifuged at 1,500 rpm for 5 min. In this study, isotype antibodies were used for fluorescence minus one control and confirmed negative population of antibodies. An automatic hematology analyzer (Sysmex Corp., Kobe, Japan) was used to obtain the absolute cell counts of lymphocyte subsets (Lee et al., 2022a). Flow cytometry in this study was used to measure the distribution of CD4-positive helper T-cells, CD56-positive NK cells, and CD8-positive cytotoxic T-cells (Park et al., 2021).
Walking programs
The schedules for walking program took place at the following times: SWG at 10:00, MWG at 14:00, and FWG at 16:00, respectively. As opposed to the exercise groups participating in the walking program, CON mediated or lightly stretched while lying down for 30 min on a mattress during their scheduled time, recommending not to participate in any other aerobic exercise. Before participating in the walking program, all subjects did a warm-up exercise for 5 min, and after the walking program was over, they laid down on the mattress and did a cool-down exercise for 5 min. Treadmill walking program conducted on 30 min a day, 5 per week. Walking program performed for 12 weeks, and the walking speed was set based on ratings of perceived exertion (RPE). The reason why self-awareness is set as exercise intensity is that it is generally recommended to set RPE as walking intensity because it is difficult to set the intensity based on heart rate and it is not accurately measured in the presence of chronic diseases (Julius et al., 2012). RPE 20 scale was applied referring to the RPE range suggested in the previous study and SWG was encouraged to walk in the RPE 8–10 range, MWG in the RPE 11–13 range, and the FWG 14–16 RPE range. Three groups were asked to walk at a very slow initial treadmill speed for about 3 min before entering the set RPE intensity. Observers kept their eyes close to the treadmill while the subjects walked. If the walking gait becomes abnormal or if the walking does not match the speed, the speed was lowered. However, it was requested that the set RPE be kept, and the researchers observed it.
Data analyses
GraphPad Prism 9.3.1 (GraphPad Software, San Diego, CA, USA) were used for data analysis. All data are presented as mean± standard deviation. The Shapiro–Wilk test was used to evaluate demographic and anthropometric measures for normality. Prior to the full-scale analysis, this study analyzed the prelevels of the variables using the Kruskal–Wallis test to search for any baseline differences. Comparisons of variables were conducted with nonparametric Kruskal–Wallis test and adjusted for multiple comparisons. For detailed data analysis, each period was calculated as delta (Δ) %. Changes of the pre- and postvalues for specific variables were confirmed using the Wilcoxon signed-rank test. Cohen d was used to find the effect size (η2), which equals the groups’ mean difference divided by the pooled standard deviation (Cohen, 1992). Statistical significance was set at P≤0.05.
RESULTS
Demographic and controlled variables
The minimum age of subjects was 65 years, and the maximum age was 78 years. The mean age was 71.75±3.52 years with no significant difference in the age ranges of the four groups. There was no significant difference between the four groups in terms of demographic and physical characteristics before the experiment. Specifically, body mass index (BMI) before the start of the experiment was 26.43±2.69 kg/m2 in CON, 25.12±1.31 kg/m2 in SWG, 26.64±2.63 kg/m2 in MWG, and 26.72±3.12 kg/m2 in FWG. This BMI levels of the four groups were between ‘Preobesity’ and ‘Class I obesity’ (Kim et al., 2021). It was not significantly different between the groups (P=0.513; η2=0.070).
As shown in Fig. 2, the muscle mass of CON, SWG and MWG decreased, whereas that of FWG increased significantly in Wilcoxon signed-rank test. In detail, the muscle mass of CON before the experiment was 33.93±2.93 kg but decreased to 32.98± 3.04 kg after the experiment (Δ=−2.79%±3.69%, P=0.068). In the case of SWG, it was 34.74±2.04 kg, but it was reduced to 34.59±1.88 kg (Δ=−0.40%±1.30%, P=0.326) at week 12. In MWG, it was 35.77±2.42 kg at the baseline, but it was 35.74± 3.73 kg (Δ=−0.24%±6.13%, P=0.889) at week 12. On the other hand, the muscle mass of FWG was 32.03±4.13 kg before the experiment but it increased to 32.34±3.27 kg (Δ=1.31%±4.22%, P=0.624) in the end of experiment. That is, while the percentage of change in muscle mass decreased in the three groups, it increased only in FWG, but there was no significant difference (P=0.292, η2=0.122) between the groups.
Daily caloric intake at baseline month was 1,459.63±550.34 kcal in CON, 1,526.38±744.38 kcal in SWG, 1,192.63±444.42 kcal in MWG, and 1,603.88±307.56 kcal in FWG, showing no significant difference (P=0.361, η2=0.087) between the groups. After 12 weeks, it was 1,497.25±404.91 kcal in CON, 1,498.63± 764.41 kcal in SWG, 1,411.38±422.03 kcal in MWG, and 1,532.63±311.79 kcal in FWG, showing no significant difference (P=0.787, η2=0.009) between the groups. The daily amount of physical activity at baseline month was 1,498.13±242.97 kcal in CON, 1,381.25±221.68 kcal in SWG, 1,555.13±277.84 kcal in MWG, and 1,400.75±193.73 kcal in FWG, showing no significant difference (P=0.639, η2=0.094) between the groups. After 12 weeks, it was 1,252.75±165.04 kcal in CON, 1,415.25± 213.04 kcal in SWG, 1,495.13±282.21 kcal in MWG, and 1,340.00±194.16 kcal in FWG, showing no significant difference (P=0.270, η2=0.162) between the groups.
Changes and differences of muscle contractility
As shown in Table 2, the Tc of dominant BF decreased in CON and SWG but increased in MWG and FWG after 12 weeks. As a result of the post hoc test on the change rate, it was found that the FWG increased the most, followed by the Tc of the MWG. This tendency was similarly observed in Tc of nondominant BF. In Wilcoxon signed-rank test for total Tc of BF as shown in Fig. 3A, CON and SWG decreased or remained unchanged, whereas MWG and FWG increased significantly.
At the end of the experiment, Tc of dominant RF decreased in CON and SWG, but increased in MWG and FWG. In the posttest results of the rate of change, the Tc of FWG was the highest, followed by MWG, SWG, and CON sequentially. This trend was similar to Tc of nondominant RF. Meanwhile, the total Tc of RF as shown in Fig. 3B, CON and SWG decreased significantly, whereas that of MWG was not significantly changed. However, that of FWG increased significantly after 12 weeks.
Although the Dm of dominant or nondominant BF increased in CON and SWG, those decreased in MWG and FWG as shown in Table 2. In the posttest results of the rate of change, Dm of FWG was the lowest, and MWG, SWG, and CON were sequentially shown. A similar trend was also observed in RF. In Wilcoxon signed-rank test for total Dm of BF as shown in Fig. 3C, those of CON and SWG increased, whereas those of MWG and FWG decreased significantly. As shown in Fig. 3D, although the total Dm of RF of CON and SWG showed a significant increase, those of MWG and FWG showed a significant decrease.
Changes and differences in immunocytes
As shown in Table 3, although the leucocyte of CON and SWG showed a tendency to decrease after 12 weeks, those of MWG and FWG showed a tendency to increase. In the case of neutrophil, that of CON decreased, while there was no change in SWG and increased in MWG and FWG, respectively. However, lymphocyte showed a tendency to decrease in CON and SWG, but an increase in MWG and FWG.
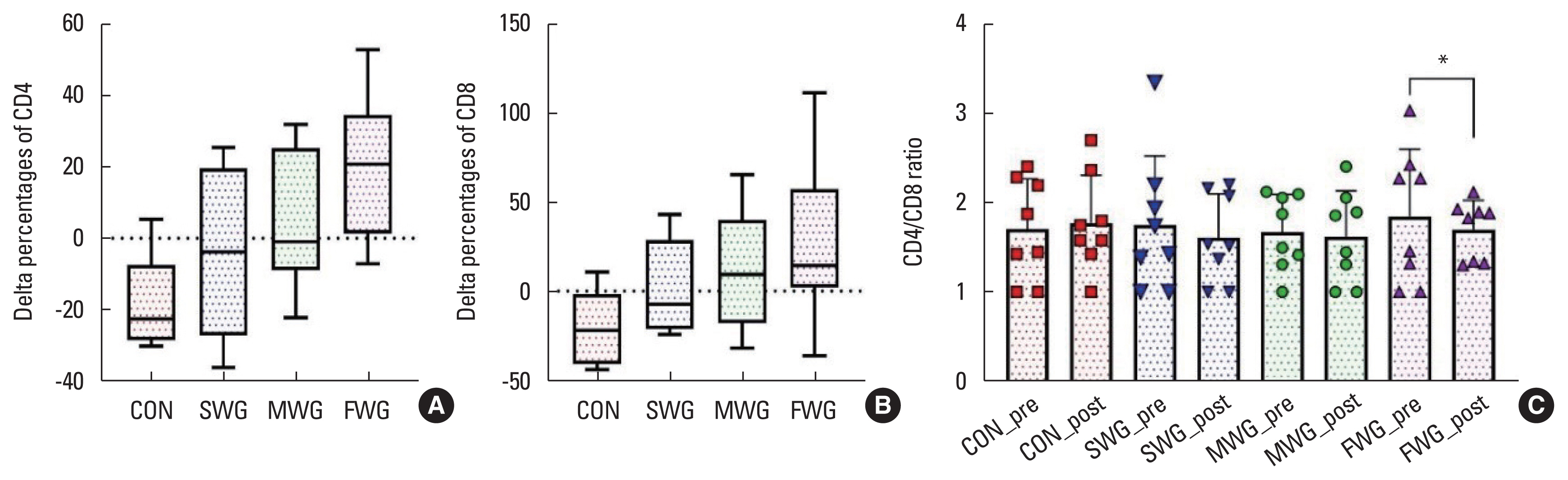
Although the helper T cell decreased in CON and SWG, those of MWG and FWG increased. Similarly, the cytotoxic T cell of MWG and FWG were improved after the experiment compared to before the experiment as shown in Table 3. In the case of NK cells, CON showed a tendency to decrease, while SWG and MWG showed a tendency to increase, but neither showed a significant change. However, the NK cell level of FWG showed a significant increase, demonstrating the effectiveness of walking fast. It can be also observed that fast walking was significantly reduced the CD4/CD8 ratio as shown in Fig. 4.
DISCUSSION
The primary outcome of this study was moderate or higher intensity maintains muscle mass and improves muscle property in the elderly women. The secondary outcome was walking at moderate to high intensity produced positive changes in some immunocytes including neutrophil, helper T cell, and NK cell. These results suggest that even elderly women who are vulnerable to sarcopenia can prevent muscle loss and do not lower their immune function if they walk over moderate intensity.
Although fast walking in this study was not statistically significant, it did not decrease muscle mass in elderly women. Muscle mass of the CON not participating in the walking exercise decreased by ~3%, while the SWG and MWG decreased by ~0.4% and ~0.2%, respectively. However, the muscle mass of the FWG increased by ~1.3% as shown in Fig. 2. These results suggest that brisk walking can prevent sarcopenia by maintaining a certain amount of muscle mass in elderly women. In fact, since sarcopenia is a very important issue for the elderly, various organizations around the world are issuing recommendations for this. As an example, the European Working Group on Sarcopenia in Older People has proposed a revised protocol for the definition of sarcopenia: muscle performance and muscle quality take higher classification importance (Cruz-Jentoft et al., 2019). Timed up and go test has been adhered to as a method for examining this sarcopenia (Soubra et al., 2019), but recently it has been reported that TMG can also differentiate sarcopenia (Fabiani et al., 2021). As a result of measuring the muscle properties of the elderly after 12 weeks of the experiment through this TMG test, the Tc levels of the groups that did not participate in the walking program or walked slowly decreased, while the Tc levels of the groups that performed moderate or more walking increased significantly. That is, Tc of dominant and nondominant BF decreased in CON and SWG but increased in MWG and FWG after 12 weeks. This tendency was similar to Tc of dominant and nondominant RF. In this context, Macgregor et al. (2018) have reported that the Tc has a very high correlation with the proportion of the slow twitch muscle fibers. It is highly likely that the slow twitch muscle fibers are stimulated to some extent and these fibers increase after a certain period. However, the results of this study found that it is possible to maintain or increase slow twitch muscle fibers at a certain walking speed. In addition, it can be inferred that strong-intensity walking can maintain fast twitch muscle fibers even if the exercise type is aerobic exercise. This is because, regardless of the type of exercise, how the target person tries to cope with the exercise is important. In other words, this is because the Tc and Dm of elderly women who performed moderate or more walking in this study showed the characteristics of strength training.
In the case of the elderly, it was confirmed that walking at a high speed is important for the development of muscle property of the lower extremities. Changes in muscle contractile properties associated with peripheral fatigue have been extensively studied in the time domain analysis of evoked single twitch. When twitch amplitude increases because of post-activation potentiation, the recorded TMG amplitudes also increase (Julius et al., 2012), which may (Hamada et al., 2000) or may not (Petrella et al., 1989) be accompanied by increased twitch speed. That is, a correct interpretation of Tc after TMG measurement is required, and it is also necessary to study whether the examination after how much rest after exercise accurately reflects muscle properties. In addition to Tc, this study also analyzed Dm to investigate muscle characteristics. Dm stands for vertical distance that the curve reaches to the peak due to the displacement of muscle formed by muscle contraction. If there is muscle dystrophy in the elderly, it is reported to increase, whereas it is reported to decrease when muscle tension or stiffness increases (Park, 2020). Pisot et al. (2008) reported that 35 days of bed rest resulted in a decrease in muscle thickness, which was interpreted as an increase in Dm. This reduced muscle mass would have reduced muscle stiffness to allow for greater Dm in response to the stimulus (Reeves et al., 2005). This negative correlation between muscle thickness and Dm indicates a lower muscle resting tension, resulting from muscle atrophy. In this regard, this study was able to observe the change in Dm of four types of walking. That is, although the Dm of BF and RF increased in CON and SWG, they decreased in MWG and FWG after the 12 weeks of experimentation. In the posttest results of the rate of change, Dm of FWG was the lowest, and MWG, SWG, and CON were sequentially shown. These results can be considered as changing only the metabolic ability of the muscle without causing a large change in Dm (Loturco et al., 2015), even when walking fast due to the characteristics of the elderly. In most studies so far, it is reported that the muscle properties change after a certain exercise, and the Dm of TMG decreases in comparison to the CON, which indicate that Dm decreases because the muscles of the exercised person become harder than those of the persons who do not perform the exercise, resulting in increased stiffness and muscle tone (Zubac and Šimunič, 2017).
Alterations in the human body according to regular exercise can improve or maintain health-related fitness (Caspersen et al., 1985) and provide ancillary effects in addition to the changes in Tc and Dm of TMG investigated in this study. In other words, improvement of muscle mass as well as muscle property through a regular walking positively changes immunocytes function to exert a protective effect on the human body (Lee et al., 2022b). According to many reports, aging increases inflammation-inducing factors along with a decrease in immunocytes, T cell and NK cell (Allman and Miller, 2005; Linton and Dorshkind, 2004). Several previous studies also reported that the changes in leukocytes and leukocyte subtypes as a result of aging lead to decreased immunocytes function but exercising regularly can maintain and improve immunity in the elderly (Lee et al., 2022b; Tvede et al., 1989).
Similar to previous studies, the main findings from this study also found that regular walking improves immunocytes function in elderly women. A characteristic fact is that most of the immunocytes were not significantly different in the CON and the SWG for 12 weeks. These results can be interpreted that walking at a slow speed does not provide a positive effect on immunocytes of elderly women. In addition, neutrophil, which have strong phagocytic action on foreign substances, did not change in CON, whereas the three walked groups showed a tendency to increase. Specifically, the helper T cell and NK cell showed a marked increase only in FWG compared with other groups. Moreover, fast walking reduces the CD4/CD8 ratio, which could increase susceptibility to infections (Ramel et al., 2003) due to an increase in a small amount of helper T cell (CD4+) and a greater amount of cytotoxic T cell (CD8+) in this study. These results can be interpreted that although over moderate-intensity walking provides a positive effect on immunocytes, the response and adaptation of various immunocytes to exercise are different. Single bouts of moderate-intensity exercises provide enhancing effects on immunity used to improve vaccine responses in “at-risk” patients. Some of the benefits to immunity from exercising regularly at moderate intensity include enhanced immunosurveillance, composition changes of “older” and “younger” immunocytes (Simpson et al., 2015). Campbell et al. (2009) also reported that vigorous exercise could increase NK cell concentration tenfold compared to low-intensity exercise. Conversely, Gleeson (2007) suggested that regular moderate levels of exercise is reduces the incidence of infection compared to being completely sedentary. However, they also suggested that prolonged bouts of strenuous exercise led to a temporary reduction of immune function. Although many studies have suggested the effect of exercise to improve the immune function of the elderly, they still present different results depending on the intensity, duration, and type of exercise. In particular, it does not suggest how much intensity of walking that can be performed without a special tool brings desirable results to immune cell function. The main causes of exercise-related the changes of immunocytes depend on the intensity, duration, and fitness level of the exercise. In addition, the body’s immune cells can be affected by exercise depending on age. However, the mechanism of immunocytes increase due to exercise has been found to occur as a result of an increase in cardiac output, a hemodynamic factor, hemoconcentration caused by an increase in extracellular fluid during exercise, and an increase in epinephrine (McCarthy et al., 1988). The above mechanism of exercise improves the activity of cells and provides smooth help to the immunocytes function that protects the human body, so it is important to make an effort to be a steady exercise even for the elderly.
This study revealed the benefits of moderate-to-high-intensity walking on immune function by enhancing the muscle mass and muscle property of the thighs and by improving the overall fat levels of the elderly women. However, this study has some of the limitations that include a small sample size and limited diversity in terms of demographic and chronic disease background. As such, we encourage future researchers to include a larger and more diverse pool of subjects, and to observe a greater number of immunocytes.