INTRODUCTION
Strengthening the hip extensors, such as the gluteus maximus (GM) or hamstring, is a long-standing staple of the sports and rehabilitation fields (Al Attar et al., 2017). Such exercises prevent sports injuries, enhance recovery after injury, and increase athletic performance during physical activities (Bourne et al., 2015; van Dyk et al., 2017). Specifically, increasing hamstring strength can reduce the compressive force on the knee joint and decrease excessive anterior tibial translation (Al Attar et al., 2017; Whyte et al., 2019). During recovery, especially for an anterior cruciate ligament injury, hamstring-strengthening exercises are an important intervention against anterior shear forces in the knee joint (Cheung et al., 2012). For athletes such as sprinters, initiating a sprint requires greater contractions of the hip extensors. Despite their clear importance, exercises to strengthen hip extensors have been studied considerably less than those to strengthen hip flexors or knee extensors.
Clinical literature has suggested several strengthening exercises for the hamstring and gluteal muscle groups, including the hamstring curl, single-leg extension, Roman chair exercise, and Nordic exercise (McAllister et al., 2014; Park and Yoo, 2014; van Dyk et al., 2017). Recent findings have demonstrated the biomechanical effectiveness and practical benefits of the Nordic exercise (van Dyk et al., 2019; Whyte et al., 2019). This exercise (also called the “Russian hamstring exercise”) can be performed with a partner without any substantial equipment (Ebben, 2009). Although previous studies have noted several advantages of the Nordic exercise (Ebben, 2009; McAllister et al., 2014; van Dyk et al., 2019; Whyte et al., 2019), few reports have investigated variations of this exercise.
Changes in the base of support or variations in the exercise angle can affect exercise effectiveness and the activation of particular muscles. For example, Park and Yoo (2014) reported that changes in support angle during the Roman chair exercise differentially activated muscle groups in the lower extremities. During hamstring curl exercises, changes in knee angle stimulated the knee extensor and hip extensor muscles. Thus, selective activation of a specific muscle can be accomplished by applying small changes in a given exercise. To the best of our knowledge, however, there are a few studies considering parameter changes in the Nordic exercise (Hegyi et al., 2019; Narouei et al., 2018). Narouei et al. (2018) reported that the coactivation of trunk muscles and muscles of the lower extremities is important during eccentric and concentric Nordic exercises. Hegyi et al. (2019) demonstrated that higher knee extensions can maximize the strengthening effects of the exercise. However, the effects of varying other Nordic exercise parameters remain unstudied; therefore, it is necessary to investigate whether adjustments to this exercise can be used to selectively activate specific muscles.
The present study hypothesized that the magnitude of knee flexion during the Nordic exercise would significantly influence exercise effectiveness, which could be modulated by the inclination angle during the Nordic exercise and the base slope angle. The purpose of the present study was to investigate the muscular activity of the lower extremities during Nordic exercise variations based on adjustments to the inclination angle and base slope angle.
MATERIALS AND METHODS
Participants
By using a convenience sampling, participants were recruited from a local university. The sample size in present study was determined using G-power 3.1.3 software (University of Dusseldorf, Dusseldorf, Germany), which was set as two-way of repeated measure design, a significant level of 0.05, power of 0.8. As an inclusion criterion, it was determined as participant with no musculoskeletal disorder during recent 6 months. For reducing the bias of the gender differences, and concerns of the disturbing signal due to fat tissue, present study has performed with the male participants who were less than 25 body mass index. Final samples of 21 males participated in this study. The height and weight of the final sample populations were 173.57±4.71 cm and 67.10±6.84 kg, respectively. The average body mass index was 22.30±2.45 kg/m2. All participants gave informed written consent according to the protocol approved by Kaya University Faculty of Health Science Human Ethics Committee (Kaya IRB-273).
Instrumentation
Surface electromyography (sEMG) data were collected using a surface EMG device (QEMG-4/LXM3204, LAXTHA, Daejeon, Korea). The sEMG signals were sampled with a 1,000 Hz frequency. The data obtained were computerized with the EMG acquisition software (Telescan 2.89, LAXTHA, Daejeon, Korea). The band-pass (20–450 Hz) filter (60 Hz) was used. Four channels of surface electrodes were attached on the dominant right side of the each subject. An electrode of lumbar level of erector spine (ES) muscle was attached to a site at belly of the ES which level of 3rd lumbar spine, an electrode of GM muscle was attached to half the distance between the trochanter and sacral vertebrae in the middle of the muscle, an electrode of biceps femoris (BF) muscle was attached to a site at two-thirds of the distance between the trochanter and the back of the knee, an electrode of gastrocnemius (GCM) muscle was attached to a site running parallel to the muscle fibers, 2 cm lateral to the midline (Hermens et al., 2000). A ground electrode was placed on the lateral malleorus. The skin surface was shaved if the skin surface is covered with hair, then the skin was cleaned with alcohol. After attaching the electrodes, signal check has been performed to get a good electrode-skin contact. For identifying the subjective difficulties of each exercise, the Borg rating for perceived exertion score (Borg RPE score 6–20) was investigated after performing each exercise (Scherr et al., 2013).
Procedures
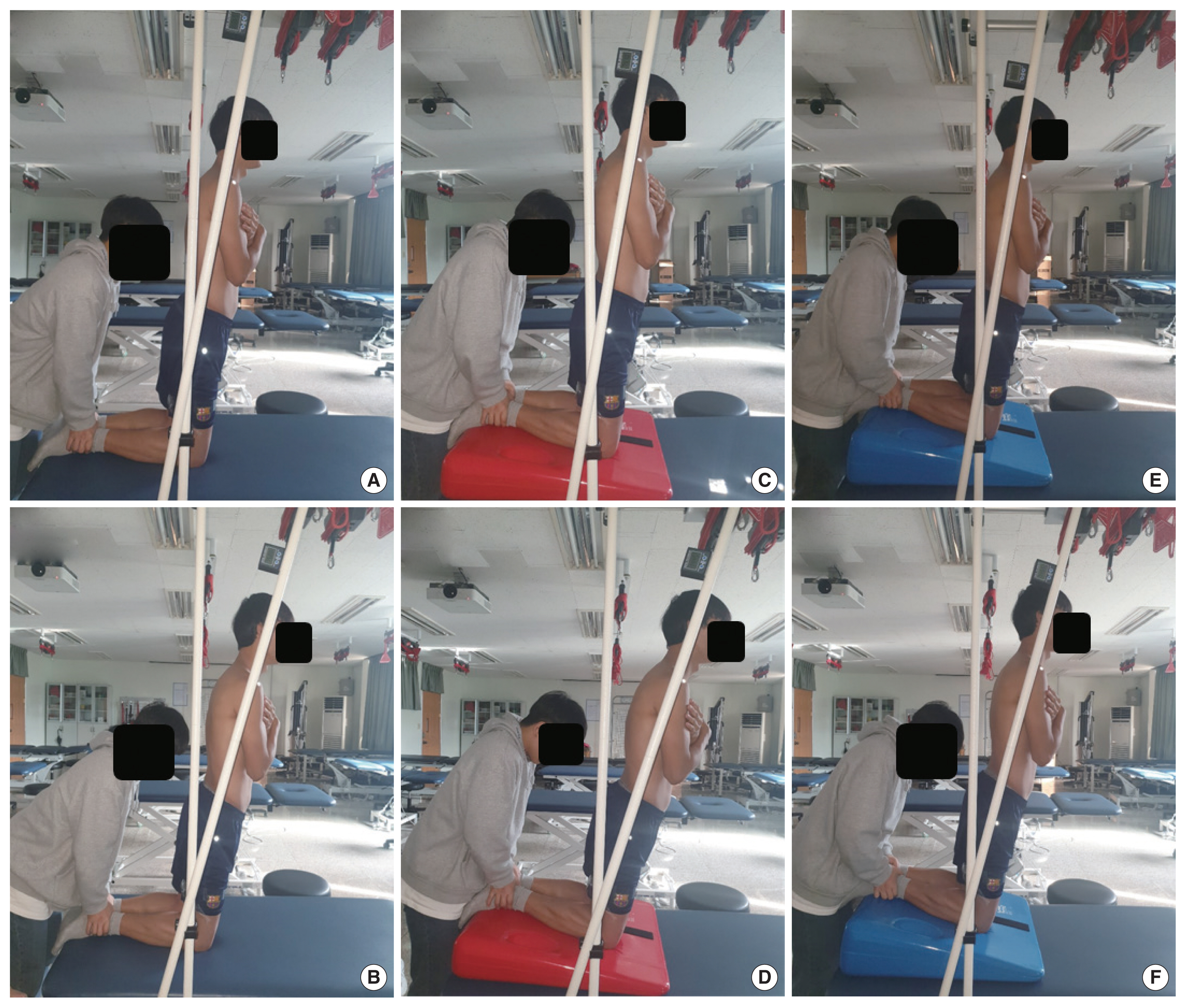
After 10 min of practice and rest time for acclimation to the exercise, the subject performed the Nordic exercise. Two Nordic angles (10°, 15°) and three base slope angle (0°, 5°, 10°) were included as the Nordic exercise conditions in present study (Fig. 1). As the starting position, the subjects were in the kneeling position with upright state of trunk, the ankle joint was fixed with secondary researcher who wears the latex glove not to distract the sEMG signal. Each subject lowered whole of the trunk forward to the ground until slant angle pointing 10° and 15°. The angle of the Nordic exercise angle was controlled by the poll with the inclinometer. Base slope angle was also varied at 0°, 5°, and 10°, which was controlled by the exercise wedge. If the subjects reached the target point of the Nordic exercise angle, they were instructed to not to elevate their hips, to try to maintain the pelvic tilt angle, and to maintain their position for 5 sec. The sEMG data were collected over a period of 5 sec controlled by metronome. The first and last 1 sec was eliminated, and the activity from middle of 3 sec was used for further analysis.
The participants performed two trials of each conditions of the Nordic exercise, and were allowed to rest 5 min between trials. After providing sEMG data during the Nordic exercise, each subject performed two trials at maximal voluntary isometric contraction (MVIC) for the included muscles against manual resistance (Ekstrom et al., 2007). Six Nordic exercise variations were randomly assigned, and subjective difficulty was investigated just after each Nordic exercise.
The average value between the two MVIC trials was used for the normalization procedure. The normalized values of ES, GM, BF, GCM were presented as %MVIC. The values including normalized surface EMG, Borg RPE scale values were used for statistical analysis.
Statistical analysis
The root mean square of sEMG data during the exercise was obtained with a widow length of 0.125 sec and averaged. The data are expressed as the %MVIC for the Nordic exercise. IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA) was used to determine the significance of differences in %MVIC between conditions. For identifying the normal distribution of data, the Kolmogorov–Smirnov test has been done before the statistical analysis. The two-way analysis of variance was performed to test for differences in %MVICs between the Nordic exercise variations. For the main effects derived via pairwise multiple comparisons, the Bonferroni correction was performed to identify specific differences among the three groups. In all analyses, P<0.05 was taken to indicate statistical significance.
RESULTS
The mean values of normalized EMG data and Borg RPE score data were represented in Table 1. The factor of Nordic angle differences significantly affected the normalized sEMG and subjective difficulties. The 15° of Nordic exercise showed significantly higher %MVIC value of the ES, GM, BF, GCM, and Borg RPE score, compared to the 10° of Nordic exercise (Table 1) (Figs. 2, 3) (P<0.05).
There was a significant difference in factor of base slop angle, which was varied depends on muscle. The activities of the BF and the GCM were decreased with increases of base slop angle. In the result of the BF, the significant differences were found between 0° and 10°, 10° and 15°, 0° and 15° of base slop angle (Fig. 2) (P< 0.05). Limited in 15° of Nordic exercise condition, the activities of the GCM were significantly different between 0° and 15° of base slop angle (Fig. 3) (P<0.05).
The activities of the GM and subjective difficulty (Borg RPE score) were increased with increases of the base slop angle. In the result of the GM, the significant differences were found between 0° and 10°, 0°, and 15° of base slop angle. In the result of the BF, the significant differences were found between 0° and 10°, 10° and 15°, 0° and 15° of base slop angle (Fig. 2) (P<0.05). The Borg RPE score was significantly elevated with serial increases of the base slop angle (Fig. 3) (P<0.05). The muscular recruitment of the ES showed no significant differences in factor of base slop angle (P>0.05).
DISCUSSION
This study investigated the effects of the inclination angle and base slope angle during Nordic exercise on muscular activities and subjective difficulties. During the Nordic exercises, muscles exhibited 40%–80% MVIC activity, except for the GM, which exhibited 20%–40% activity. Previous studies have reported the muscular activity during exercises intended to activate specific muscles (Akuzawa et al., 2017; Hegyi et al., 2019; Mullaney et al., 2011; Park and Yoo, 2014). For example, the heel-raise exercise for activating the triceps surae stimulates the GCM at 60%–100% MVIC (Akuzawa et al., 2017; Mullaney et al., 2011). Hegyi et al. (2019) reported that the BF is activated at 40%–85% during BF-dominant exercises. During the bridge exercise, which is widely used in rehabilitation, ES activity is reported to be approximately 30%–40% MVIC (Czaprowski et al., 2014). The Roman chair exercise reportedly activates the GM at 30% MVIC (Park and Yoo, 2014). The present results show that the Nordic exercise is appropriate for strengthening the plantar flexor of the ankle as well as the entire hip and the trunk extensors.
The angle of the Nordic exercise (i.e., the magnitude of forward movement) affected muscular activity and subjective difficulty. The fulcrum of the Nordic exercise is the knee joint, and the lever arm includes the whole upper body and the upper lower limbs (Hegyi et al., 2019). Because the Nordic exercise does not allow for trunk flexion or pelvic tilt, small increases in forward movement result in drastic increases of the internal moment of the hip extensor and knee flexor against the external moment of forward falling. This mechanical change may explain the significant increases in muscular activity and subjective difficulty observed in the present study when the exercise angle was increased from 10° to 15°.
Increasing the base slope angle also significantly affected muscular activity and subjective difficulty in the present study. Serial decreases in GCM and BF activity as the base slope angle increased might have been caused by insufficiency due to shortening. Increases in the base slope angle resulted in an increased knee flexion angle during the exercise, which might have resulted in insufficiency due to shortening of the knee flexors, including the GCM and BF (Šarabon, 2019). Conversely, GM activity increased with increasing base slope angle. During hip and trunk extension exercises, it was not surprising that the flexed knee position increased GM activity. Park and Yoo (2014) demonstrated that a flexed knee position during the Roman chair exercise increases GM activity relative to an extended knee position. Although it is difficult to confirm that the muscular compensation was due to extensive hip and trunk muscle extension, we suspect that the decreased muscular requirements of the GCM and BF may be related to increases in GM activity.
The Borg RPE scale was originally designed to measure the physical strain of aerobic exercise. However, studies have shown that RPE is also related to resistance exercise intensity (Row et al., 2012; Scherr et al., 2013). The present results show that subjective difficulty, as indicated by the Borg RPE score, increased with increasing Nordic exercise angle and base slope angle. Previous studies have warned of the difficulty of the Nordic exercise and the risk of injury, especially when adjusting the concentric and eccentric phases of the exercise protocols (Lacome et al., 2019). To prevent injury risk and allow for wider usage of the Nordic exercise, the present study established isometric exercise conditions with limited exercise and base slope angles. In a previous study, which used an RPE scale of 6–20 points, scores of 11–13 were typical for less-trained people, whereas scores of 13–15 were recommended for individuals who required more intense training (Scherr et al., 2013). In the present study, the values for the 10° Nordic exercise ranged from 11 to 13, whereas those of the 15° variant ranged from 12 to 17. In addition, increases in the base slope angle resulted in slight serial increases in subjective difficulty during the exercise. Although the limited number of subjects in the present study was not sufficient to generalize the results, we recommend a step-wise application of the Nordic exercise based on modifying the exercise and base slop angles.
The present study examined the effects of changing Nordic exercise parameters on muscle activity and subjective difficulty. The results highlighted that selective activation of muscles in the lower extremities can be accomplished by controlling the base slope angle and exercise angle while performing the Nordic exercise. However, several limitations should be addressed by future studies. The most important limitation was that the semitendinosus and latissimus dorsi, which are influenced by the Nordic exercise, could not be assessed in the present study. Second, we could not record kinetic data from the pelvic or trunk regions, thus the fixation of the pelvis could not be objectively identified.
In summary, there are two considerations when employing the Nordic exercise. First, a higher exercise angle induces higher muscle recruitment in the lower extremities. However, this should be carefully adjusted based on the individual because subjective difficulty also increased with increasing angle. Second, the base slope angle can be controlled with a base wedge during the exercise, which affects the knee joint angle. The higher slope angle induces lower recruitment of muscles in the lower extremities, such as the GCM and GM, but contributes to higher recruitment of the gluteal muscle.