INTRODUCTION
Parkinson disease is defined as a progressive neuromuscular disorder that interferes with motor pathways within the central nervous system (Kalia and Lang, 2015). Parkinson disease is the second most common degenerative disease of the central nervous system affecting 1% of the population above 60 years of age; it is predicted to increase in prevalence as the population ages (Beitz, 2014; Tysnes and Storstein, 2017). Common clinical findings of Parkinson disease include tremors, rigidity, ceasing (or “freezing”) of volitional movements, hypokinesia, bradykinesia, decreased stability limits, and a festinating gait pattern classified by abnormally slow shuffling steps with an anteriorly displaced center of mass (Massano and Bhatia, 2012). The “freezing of gait” phenomenon is a particularly debilitating component of Parkinson disease in which the voluntary muscle movements used to walk normally are inhibited, causing the patient to abruptly cease volitional movements in midstride (Heremans et al., 2013). This leads to an increased fall risk, negatively impacts independence, and consequently decreases a patient’s overall quality of life. Therefore, the development of therapies with the goal of reducing the impacts of freezing episodes on gait is crucial to the well-being of the patients, their families, and society.
Biofeedback is the process of receiving information from the body’s normal functions, often with the aid of external electronic sensors. Auditory biofeedback utilizes sound for this purpose and the use of auditory biofeedback has demonstrated the ability to improve weight-bearing symmetry during gait for individuals with lower limb injuries (Isakov, 2007). Similarly, use of combined somatosensory and audio-biofeedback for patients following a stroke has demonstrated the potential to improve step length, symmetry and speed significantly more than gait training without augmented feedback (Sungkarat et al., 2011). There is limited high-quality evidence supporting the use of rhythmic auditory cues to enhance walking speed for patients with Parkinson’s disease (Lim et al., 2005). Furthermore, it is unclear if the positive effects identified in the laboratory can subsequently lead to improved activities of daily living and a reduction of falls in the community (Lim et al., 2005). In addition, the sustainability of a cueing training program remains uncertain. More recently, Mirelman et al. (2011) conducted a pilot study with seven patients with Parkinson disease utilizing an auditory biofeedback system in which the device was worn on the patient’s belt and attached to headphones by which the patient hears the auditory feedback. These researchers concluded that audio-biofeedback training was feasible and associated with improvements in balance for patients with Parkinson disease (Mirelman et al., 2011); however, research examining the utility of audio-biofeedback specific to gait training in this population is still quite limited (Gordt et al., 2018). Thus, there appears to be a need for further efforts in the area of rhythmic auditory cueing and its influence on gait and function in patients with Parkinson disease.
A recent device that was developed called Electroskip (Electroskip LLC, Buffalo, NY, USA) produces real-time auditory biofeedback and a self-generated, trailing metronomic sound for the purpose of cueing a patient with Parkinson disease. The hardware itself is comprised of a wireless, wearable device that sends a discrete signal when the user steps on either the heel or toe force sensors. Electroskip is compatible with the musical instrument digital interface protocol allowing for a wide range of digital sounds, synthesizers or musical beats to be utilized. The metronome sound produced by the patient also adjusts in tempo-based upon the speed of the walker. This is significant as Electroskip not only generates instantaneous biofeedback, but also will serve as its own auditory cue for the following steps in the maintained time frame, which we hypothesize will address the gait speed abnormalities associated with the freezing of gait phenomenon of Parkinson disease. Therefore, the purpose of this case study was to explore the possible beneficial effects of a rehabilitation program with an audio-biofeedback technology called Electroskip in a patient with moderate Parkinson disease.
MATERIALS AND METHODS
Participant
The patient was a 61-year-old man with moderate Parkinson disease (Hoehn and Yahr Parkinson’s scale stage III) (Hoehn and Yahr, 1967) who had progressive episodes of freezing of gait. In addition to Parkinson disease, which was diagnosed 3 years prior, his medical history included dementia, depression, and hypertension. The patient’s Parkinson disease was managed with carbidopa-levodopa 4 times daily. The patient was also taking donepezil hydrochloride for dementia, citalopram hydrobromide for depression, and hydrochlorothiazide for hypertension. In addition to progressive episodes of freezing gait, the patient had a history of greater than 3 falls per every 6 months span, decreased sitting and standing balance without support, decreased upper and lower extremity strength, poor motor control and muscle sequencing, decreased upper extremity range of motion, and difficulty with dynamic balance and gait activities. While the patient also had verbal and cognitive deficits, he was alert, oriented to person and place, and he was able to follow commands necessary during rehabilitation to be an active participant in his therapy. He was accompanied by his daughter, father, and cousin, who gave written consent for participation in this case report and provided subjective information on his behalf. The patient lived with his elderly father on the first floor of a multiple story home. Family safety concerns included transferring to and from sitting to standing, transferring in and out of a vehicle, reaching overhead, stepping up/down from a curb, and safety during ambulation both indoors and outside.
Outcome measures
The outcome measures for gait and balance included the Timed Up and Go (TUG) test (Stegemöller et al., 2014), the modified Gait Abnormality Rating Scale (mGARS) (VanSwearingen et al., 1996), the modified Parkinson’s Activity Scale (mPAS) (Keus et al., 2009), the Freezing of Gait Questionnaire (FOGQ) (Giladi et al., 2000), and the Berg Balance Scale (BBS) (Berg et al., 1995). These were selected as outcome measures based on their use in prior studies with either elderly patients (mGARS, BBS) (Berg et al., 1995; VanSwearingen et al., 1996) or with patients with Parkinson disease (TUG, mPAS, FOGQ, BBS) (Giladi et al., 2000; Keus et al., 2009; Stegemöller et al., 2014). Medication dose and timing remained constant over the course of treatment and outcome measures were consistently obtained at the same time of day during the on phase of medication.
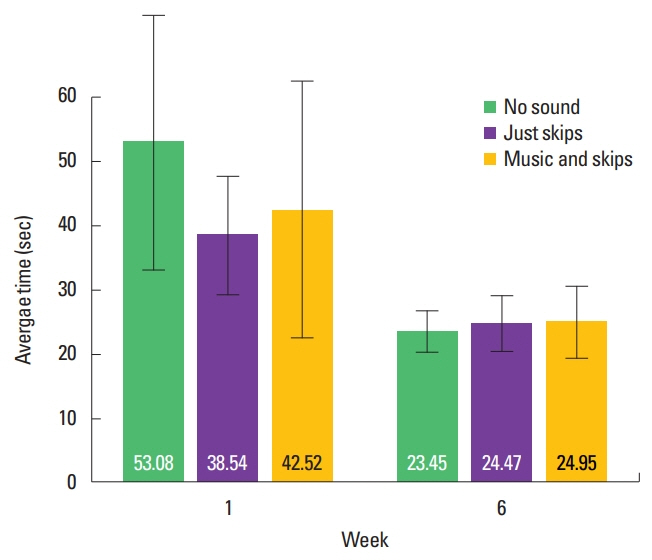
The TUG test is a timed trial assessing the time it takes for an individual to rise from a chair, traverse a 3-m distance, and return. This test was administered on testing day 1 and at the end of 6 weeks. The patient’s timed averages were collected from 5 trials each under three conditions; shoes on but sound off, shoes on with Electroskip audio-biofeedback, and shoes on with Electroskip audio-biofeedback plus an accompanying background musical track. Rest was given as needed to the patient and full recovery was ensured prior to proceeding to the next test trial. The order of the testing conditions was random on day 1 and at week 6. Every trial throughout the study began with the physical therapist positioning the patient in optimal sitting posture with consistent verbal directions for completion of the TUG task.
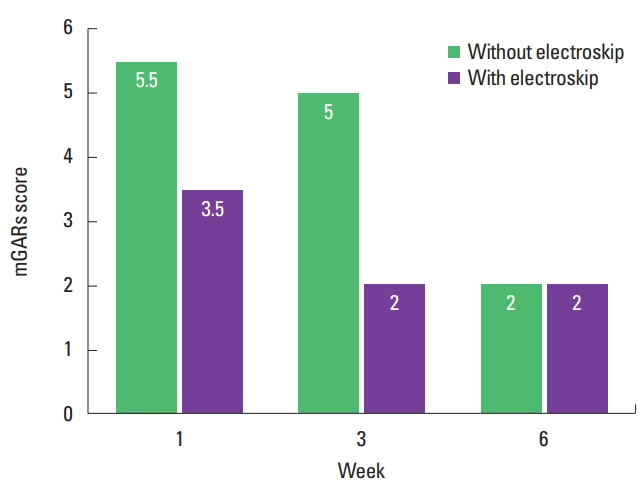
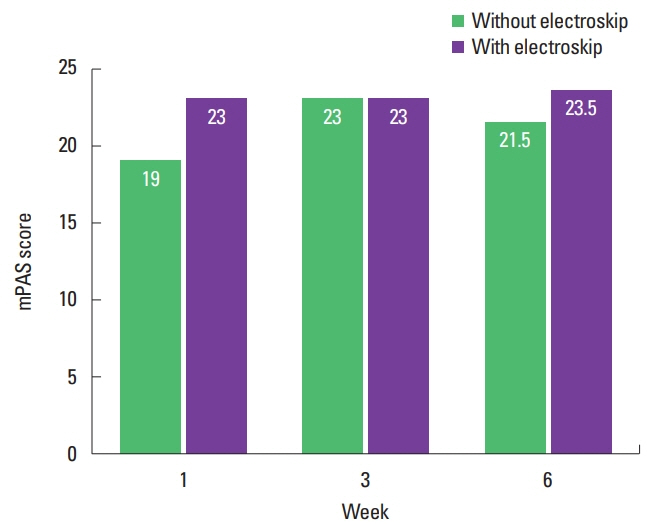
The mGARS and mPAS were administered at three points during the course of care: day 1, week 3, and week 6. The mGARS is a physical therapist scored tool in which lower scores reflect a more normalized gait pattern through observation of a 15.2-m walk and graded on certain criteria such as heel contact and variability of movements (VanSweringen et al., 1996). The mPAS (gait akinesia section specifically) is a physical therapist scored assessment in which the patient must stand up, walk a 3-m U-shaped pattern, and return to sitting under 3 conditions (i.e., without extra task, with dual task, with cognitive task), in which higher scores correspond with improved performance (Keus et al., 2009). Two trials, with and without the Electroskip audio-biofeedback, were performed at each testing trial. The order of testing was reversed at week 3 to limit effects of fatigue and learning. Both tools were scored by the lead author and then reviewed by the patient’s caregivers to ensure accuracy and to minimize bias. The mPAS was not used in full, but limited to the section pertaining to gait akinesia as the other sections were not relevant to this case.
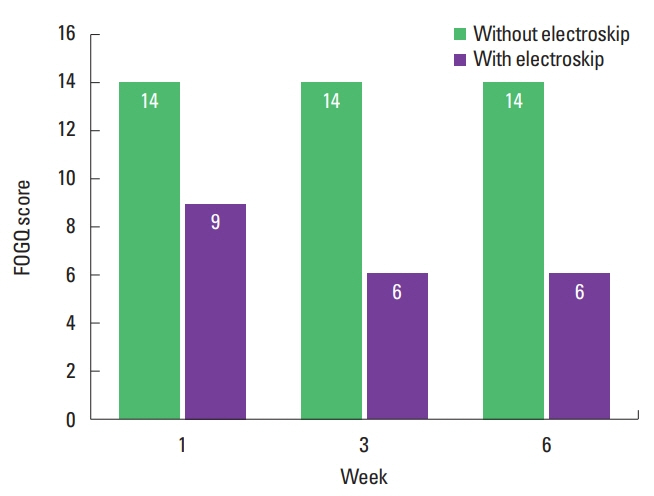
The FOGQ is a 6-question survey reflecting how freezing episodes impact a person’s gait and daily activities, in which lower scores are optimal (Giladi et al., 2000). The FOGQ, appendix B specifically, showed a strong correlation between scores achieved and quality of life amongst patients with Parkinson disease (Ellis et al., 2011). The FOGQ was given to the patients’ caregivers to complete due to the patient’s cognitive function. The questionnaire was completed on day 1, week 3, and week 6, with instructions to complete the form twice, reflecting on gait behaviors observed both with and without the Electroskip technology active during the sessions.
The BBS is a commonly used functional balance assessment tool designed to identify fall risk in community-dwelling older adults (Berg et al., 1995). It is considered the reference standard, and its use as a functional balance tool for individuals with neurologic conditions, including patients with Parkinson disease, has been well documented (Qutubuddin et al., 2005; Taghizadeh et al., 2018).
Intervention
The patient was scheduled for 3 physical therapy visits per week for 6 weeks in addition to 3 additional testing days on day 1, week 3, and again at week 6. This visit schedule is consistent with Mirelman et al. (2011), who assessed the effects of an auditory biofeedback system to augment an individualized training program on balance in patients with Parkinson disease. Physical therapy visits were 45 min and consisted of upper extremity and trunk stretching, followed by upper extremity and trunk strengthening, and concluded with functional task training (e.g., step-ups, sit-to-stand transfers, standing, kicking) and gait training (forward, backward, side stepping, turning, dual task [counting], step length cueing, arm swing normalization). Gait training utilized Electroskip technology, which is a wireless, wearable device that sends a discrete real-time generative audio-biofeedback signal when the user steps on either the heel or toe force sensors positioned under the innersoles (Fig. 1). Additionally, a self-generated metronomic sound adjusts in tempo-based upon the speed of the walker, serving as an auditory cue. The device is used by attaching two pressure sensors underneath the innersoles of the patient’s shoes (Fig. 2). A transmitter attached to the shoelaces sent wireless pulses from the sensors to a computer with audio software in order to convert the signals into audio. The biofeedback sounds were in harmony with three of the patient’s favorite songs, and the background music was included as an optional feature. When the patient would perform typical functional training, Electroskip would produce the selected tonal patterns in a steady, trailing metronomic fashion. The patient was asked to place emphasis on fluid motions that would produce a continuous and rhythmic audio-biofeedback response. The background music tracks would be used as seen fit by the therapist in order to encourage initiation of movement and participation.
RESULTS
The patient completed 17 of the 18 scheduled training sessions and all testing sessions; high satisfaction levels were reported by the patient and family after completion of the 6-week rehabilitation program. No adverse events occurred during the rehabilitation program and no falls were reported outside of the clinic by the patient or his caregivers. On day 1, the TUG test improved from 53 sec to 39 sec with the use of Electroskip technology. At 6 weeks, the TUG test was 24 sec and 23 sec with and without the use of Electroskip technology, respectively. The scores on the TUG test with the use of Electroskip technology with background music were slightly longer than with the use of Electroskip technology alone (Fig. 3). For the mGARS, scores on day 1 were 3.5/21 with the Electroskip technology and 5.5/21 without the Electroskip technology. Scores under both conditions improved to 2/21 by week 6 (Fig. 4). For the mPAS, the score was 19 on day 1, 23 at 3 weeks and 21.5 at 6 weeks without Electroskip technology; with the use of Electroskip technology, the mPAS increased to 23 on day 1 and at 3 weeks, and 23.5 at 6 weeks (Fig. 5). For the FOGQ, the score without the Electroskip technology was 14 on day 1 and it remained at 14 at weeks 3 and 6; with the use of Electroskip technology, the FOGQ decreased to 6 at weeks 3 and 6 (Fig. 6). The BBS improved from 39 days 1 to 48.5 at week 6, however, Electroskip technology was not used during assessment with the BBS.
DISCUSSION
The purpose of this case study was to explore the possible beneficial effects of a rehabilitation program with an audio-biofeedback technology (e.g., Electroskip) in a patient with moderate Parkinson disease. For the patient described in this case report, we hypothesized that Electroskip technology would address the gait speed abnormalities associated with the freezing of gait phenomenon of Parkinson disease.
This hypothesis was based upon the limited reports that have described some usefulness of audio-biofeedback with gait training in patients with Parkinson disease (Gordt et al., 2018; Lim et al., 2005; Thaut et al., 1996). Thaut et al. (1996) evaluated the effect of rhythmic auditory stimulation on various aspects of gait following a 3-week home-based gait-training program for patients with Parkinson disease. Patients who participated in the gait-training program with rhythmic auditory stimulation significantly improved their gait velocity by 25%, stride length by 12%, and step cadence by 10% more than patients who participated in a self-paced gait-training program not supplemented with rhythmic auditory stimulation, whose gait velocity improved by 7%, and patients who did not participate in a gait-training program, whose gait velocity decreased by 7%. Additionally, some features of the gait cycle as profiled with electromyography changed toward more normal muscle activation patterns for those patients who participated in the gait-training program with rhythmic auditory stimulation (Thaut et al., 1996). In our case, we did not formally assess gait parameters such as velocity, stride length, or step cadence or electromyographic activity during gait. Nonetheless, after 6 weeks of training with Electroskip technology, which combines rhythmic auditory stimulation with audio-feedback, our results seem to reflect those of Thaut et al. (1996), as improvements were observed across all testing conditions (with and without the technology active) in the majority of outcome measures used that dealt with gait. Thus, our hypothesis was generally supported.
High-quality evidence on the effects of external rhythmical cueing on gait in patients with Parkinson disease is limited. Furthermore, it is unclear whether the limited positive effects identified in the laboratory can be generalized to clinical rehabilitation programs with subsequent improved activities of daily living and reduced frequency of falls in the community (Lim et al., 2005). However, the results of this case report suggest potential immediate and short term (i.e., 6 weeks) positive therapeutic effects from the use of the Electroskip audio-biofeedback technology. While the patient described in this case report had verbal and cognitive deficits, he was alert, oriented to person and place, and he was able to follow commands necessary during rehabilitation to be an active participant in his therapy. The patient in this report subsequently performed better in every outcome during measurements taken on the first day while the technology was in use, suggesting that the patient’s motor skills received an immediate benefit from the cueing and biofeedback generated by the metronome-like sound of the Electroskip. After 6 weeks of participation in a rehabilitation program augmented with Electroskip technology, improvements were observed across all testing conditions in the majority of outcome measures used; this was most notable in the TUG test and mGAR scores (Figs. 3 and 4). This implies that the Electroskip technology may also have some benefit when used in a clinical setting for achievement of long-term rehabilitation goals. Electroskip technology, therefore, may offer a potential combination of immediate and short term (i.e., 6 weeks) clinical benefits that warrant further research into the treatment of motor impairments in patients with Parkinson disease.
For the mPAS scores, there was slightly improved performance noted with the Electroskip technology turned on in both weeks 1 and 6 (Fig. 5) compared to when the Electroskip technology was turned off. At week 3, however, the scores did not differ between those same conditions. Scores achieved without the use of the Electroskip technology increased from week 1 to 3, and then slightly decreased at week 6. Scores achieved with the Electroskip technology active showed little variation, however; they were always the same or superior when compared to the scores seen without non-Electroskip technology. The condition of the mPAS in which improvement was most notable when the Electroskip technology was enabled was when the patient was asked to perform a dual cognitive counting task while navigating the 3-m U-shaped pattern. The audio-feedback associated with the device appeared to decrease the cognitive demands on the pacing of the motor component of this task, thus allowing for the counting task to be performed with greater ease. Additionally, given the results from the other outcome measures, Electroskip technology enhanced the patient’s ability to perform smooth, voluntary motions with an immediate increase in ambulation and turning speed; the 6-week training program produced further improvements observable under all conditions.
The BBS scores from before and after the 6-week data collection period were included as supplemental data to further evaluate the Electroskip technology. Within the month prior to beginning data collection, the patient scored a 39 with their prior physical therapy program. This score increased to 48.5 after 8 weeks, which encompassed the entire 6-week duration of this study. Our results with respect to improvements in the BBS are generally consistent with those of Mirelman et al. (2011), who reported significant improvements in the BBS following a 6-week individualized training program that was augmented with auditory biofeedback in 7 patients with Parkinson disease. More specifically, Mirelman et al. (2011) reported positive trends in all measures of balance control in response to the training when subjects were assessed after the conclusion of the 6-week program. The BBS significantly improved by 3% (P=0.032) (mean pretraining score=49.0±7.2; mean posttraining score=50.4±6.7) and although not statistically significant, the TUG test scores and time to perform 5 sit-to-stand maneuvers improved by 11% (P=0.07) and 7.3% (P=0.09), respectively. These results suggest that overall balance performance may be improved following an individualized training program that has been augmented with auditory biofeedback in patients with Parkinson disease. Future trials with the Electroskip technology, or other forms of auditory biofeedback, should continue to include the BBS as a formal performance measure for more conclusive findings.
Previous research has demonstrated that visual, vibratory and auditory cueing can be effective means of overcoming a freezing episode (Velik, 2012). Cues that are both continuous and relevant to the action of stepping, such as those produced by the Electroskip, have also been found to delay the onset of freezing by engaging sensorimotor circuitry and bypassing the basal ganglia (Young et al., 2016). The potential to use auditory cues for more lasting improvements was investigated by Plotnik et al. (2014), who trained individuals with Parkinson disease to respond to rhythmic auditory stimulation immediately prior to stimuli known to trigger freezing episodes and demonstrated reduced episodes of freezing, improved gait speed and performance even when cues were removed. While this type of motor learning training may be beneficial, it requires extensive set-up of the environment to produce triggered stimulation. By combining this type of auditory stimulation with audio-biofeedback and translating this intervention into a wearable technology, the Electroskip was able to yield similar reductions in freezing episodes while wearing a device that was highly portable and worked flexibly within the clinic environment. Improvements in freezing, in this case, were not found to persist when the device was turned off as they did in previous investigations; however, it is likely the subject’s cognitive involvement limited his potential for motor learning. The subject did demonstrate improvements in gait speed on the TUG test over the course of treatment using the Electroskip that persisted when the device was removed. Walking with rhythmic auditory cueing has been previously found to improve gait cadence, velocity and stride length (Spaulding et al., 2013) and the results of this case study indicate that repeated training with audio-biofeedback during gait may have a similar beneficial training effect that can carry over to uncued gait.
There are some limitations to this report that should be considered. First, because this was a single subject case report, cause and effect cannot be inferred and the conclusions that can be drawn are limited. Observable benefits may not be generalizable to other patient populations. Second, considerable care was taken to develop the testing protocol in an individual with freezing episodes and great variability in gait. However, we are not completely sure of the effect of fatigue and motor learning on our testing protocol. Furthermore, placebo response rates may be high for patients with Parkinson disease (Diederich and Goetz, 2008). Subsequent trials are needed to determine optimal testing strategies that control for fatigue and motor learning factors, as well as possible placebo effects. However, a case series or a small open-label trial would have clinical merit and could serve as the next logical step for investigating the effects of Electroskip technology. Third, the patient had limited verbal and writing/reading comprehension skills, which likely interfered with a true self-assessment on the FOGQ. For this reason, the patient’s caregivers completed the instrument to the best of their ability and in agreement with one another. This strategy may not be optimal to assess true gait improvements, especially when they were asked to reflect on gait behaviors observed with the Electroskip technology active during the sessions, as the FOGQ is typically completed based of freezing behavior in past week. Additionally, the Electroskip technology was unavailable to the patient at home, so any comparisons of the patient’s gait with and without the technology on had to be done at similar times of the day and under similar circumstances to ensure accuracy and thus, may not reflect home use performance or the influence of the technology on activities of daily living.
In conclusion, the results of this case report suggest that a rehabilitation program focused on functional tasks, balance, and gait training using the Electroskip technology may be beneficial for improving gait and balance in a patient with moderate Parkinson disease. Future work is needed to determine the effectiveness of Electroskip technology by means of randomized controlled trials.