INTRODUCTION
High active antiviral therapy (HAART) significantly decreased morbidity and mortality related to acquired immune deficiency syndrome (AIDS) as well as improved the quality of life related to health and life expectancy in this population (Schwarcz et al., 2013). Meanwhile, a considerable proportion of people living with human immunodeficiency virus (HIV)/AIDS (PLWHA) are insufficiently active (Vancampfort et al., 2018). In addition, it is known that in advanced stages of the disease the individuals have a strong association with low levels of physical and activity capacity, although functional capacity as a predictor of morbidity and mortality has not yet been demonstrated in PLWHA (Olsen et al., 2015).
Cardiorespiratory fitness is the main variable of functional capacity and is usually assessed through the peak oxygen uptake (VO2peak) evaluated by the cardiopulmonary exercise test (CPX) (Stringer, 2010). Additionally, other variables related to integrity and capacity cardiovascular (maximal heart rate [HRmax], oxygen pulse, heart rate recovery [HRR] and half-time of the recovery maximal VO2 [T½ VO2]), and ventilatory efficiency (minute ventilation to carbon dioxide production [VE/VCO2 slope]) (Tabet et al., 2003), oxygen uptake efficiency slope (OUES) (Baba et al., 1996) also may be obtained in CPX. However, to our knowledge, these variables have not been yet evaluated in PLWHA and compared to healthy individuals.
Moreover, the CPX may be applied in physical exercise prescription using the gas exchange threshold (GET) and respiratory compensation point (RCP) (Balady et al., 2010). These parameters are important to evaluate the individual physical condition and consequently an accurate prescription for a supervised physical exercise can be done to promote functional enhancement and chronic degenerative disease prevention (Haskell et al., 2007), a condition of increasing prevalence among PLWHA (Metkus et al., 2014).
The aim of this study was to verify and to compare the responses of the cardiopulmonary variables to the incremental test in physically inactive PLWHA with well-controlled disease and physically inactive non-HIV/AIDS subjects using the CPX for cardiorespiratory capacity assessment and aerobic exercise prescription in PLWHA.
MATERIALS AND METHODS
Study design and participants
This was a cross-sectional study. The participants of the PLWHA group were recruited from a Public Health Center in Southern Brazil. This group was composed of subjects with a confirmed diagnosis of AIDS on a stable HAART regimen for at least 6 months before enrollment. A viral load below 50 copies/mL and the absence of opportunistic diseases related to AIDS were considered as well-controlled disease. Non-HIV/AIDS subjects with similar age, gender, body mass and height, without any diagnosed diseases, were recruited for convenience to compose the control group. Both, the PLWHA and control groups should not have practiced any exercise regularly for, at least, 6 months before the beginning of the tests protocol and were between 18 to 59 years of age. Exclusion criteria were based on previous history of neurological disease, tobacco and/or drug use, usage of medication with negative chronotropic action, physical and/or mental disability and pregnancy. Furthermore, if participants did not achieve at least 85% of the predicted HRmax [208–(0.7×age)] (Tanaka et al., 2001) and/or a respiratory exchange ratio (RER) of at least 1.1, they were also excluded from the study (Balady et al., 2010).
HAART regimens, HAART time use and clinical data from PLWHA were obtained from previous medical records. All patients provided an informed written consent and the study was approved by the Universidade Federal de Ciências da Saúde de Porto Alegre Institutional Review Boards (No. 951/09) and was in accordance with the Declaration of Helsinki. The study was recorded in Brazilian Clinical Trials Registry (No. RBR-7FNBZ7).
Cardiopulmonary exercise testing (CPX)
The CPX was performed using a ramp protocol on a treadmill (Centurion 300, Micromed, São Paulo, Brazil) in an environmentally controlled laboratory (temperature between 18°C–22°C and relative air humidity at around 40%–60%). Exercise test started at 3 km/hr and 0% slope, and both, treadmill speed and slope were increased gradually until the participant’s exhaustion. The exercise load was incremented individually for each participant considering their physical condition. The workload test was designed to obtain VO2peak within 8–12 min followed by one minute of active recovery (3 km/hr, 0% slope) and 5 min of passive recovery. The test was interrupted: (a) when the participant requested; (b) when the RER was >1.1; and/or (c) when a VO2 plateau was observed with an increasing workload (Balady et al., 2010). Ventilatory and metabolic parameters were collected breath-by-breath using Metalyzer 3B (Cortex, Leipizig, Germany) and were analyzed after averaging the data over 8 respiratory cycles (Neves et al., 2014). The CPX system was calibrated before each test with respect to airflow, O2 and CO2 analyzers. A 3-lead electrocardiogram was recorded using ErgoPC Elite 3.3 (Micromed, São Paulo, Brazil) at rest and during the test.
The average of the last 30s data points from the test were used to determine the VO2peak, VE, HRmax (Balady et al., 2010) and oxygen pulse (Stringer, 2010). Two independent evaluators determined the GET (Higa et al., 2007) and RCP (Balady et al., 2010). OUES (Baba et al., 1996) and VE/VCO2 slope (Sun et al., 2002) were calculated from the second minute of test until the RCP. Predicted maximal VO2 specific for Brazilian population (Almeida et al., 2014), OUES (Hollenberg et al., 2000) and VE/VCO2 slope (Sun et al., 2002) values were obtained using a previously described equation.
The HRR after exercise was assessed into two stages: (1) the first minute was undertaken at a treadmill walking speed of 3 km/hr and at 0% slope (HRmax – heart rate at 1 min of recovery), and (2) during the second minute of passive recovery (HRmax – heart rate at 2 min of recovery) (Vicente-Campos et al., 2014). Half-time of the recovery VO2peak (T½ VO2) was defined as the time from the end of the exercise test up to the point when VO2 had dropped to 50% of the final exercise value (Cohen-Solal et al., 1995).
Immunologic and virologic characteristics
To characterize PLWHA group, a blood sample (4 mL), after a 12-hr fasting period, was collected 48 hr before the exercise protocol. T CD4+ and T CD8+ lymphocytes were quantitated by flow cytometry, using FACSCalibur TM system (BD Biosciences, Franklin Lakes, NJ, USA). Viral load (bDNA) was measured by the VERSANT HIV-1 RNA 3.0 Assay (Siemens, Munich, Germany).
Data analyses
Data was analyzed using descriptive statistical techniques (measures of central tendency and dispersion). Data are expressed in median (range). The normality of the data distribution was assessed by the Kolmogorov–Smirnov test. Due to the nonparametric nature, the Mann–Whitney test was used to compare the PLWHA and the control groups, and Spearman correlation were used to examine the linear association between CPX variables. Statistical significance was defined as P≤0.05. The GraphPad Prism ver. 5.00 (GraphPad Software, La Jolla, CA, USA) was used for statistical analysis.
RESULTS
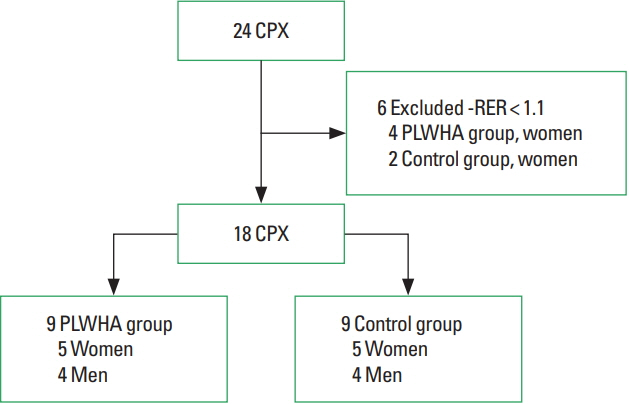
The study flowchart is presented in Fig. 1. Twenty-four participants were screened. Thirteen PLWHA (9 women) and 11 controls (7 women) composed the initial sample. However, four women from the PLWHA group and two from the control group were excluded from the data analyses because to the maximal physiologic effort (RER<1.1).
No difference in age, sex, body mass, height and body mass index (Table 1) were shown between groups. The clinical characteristics and HAART data from the PLWHA group is also present on Table 1.
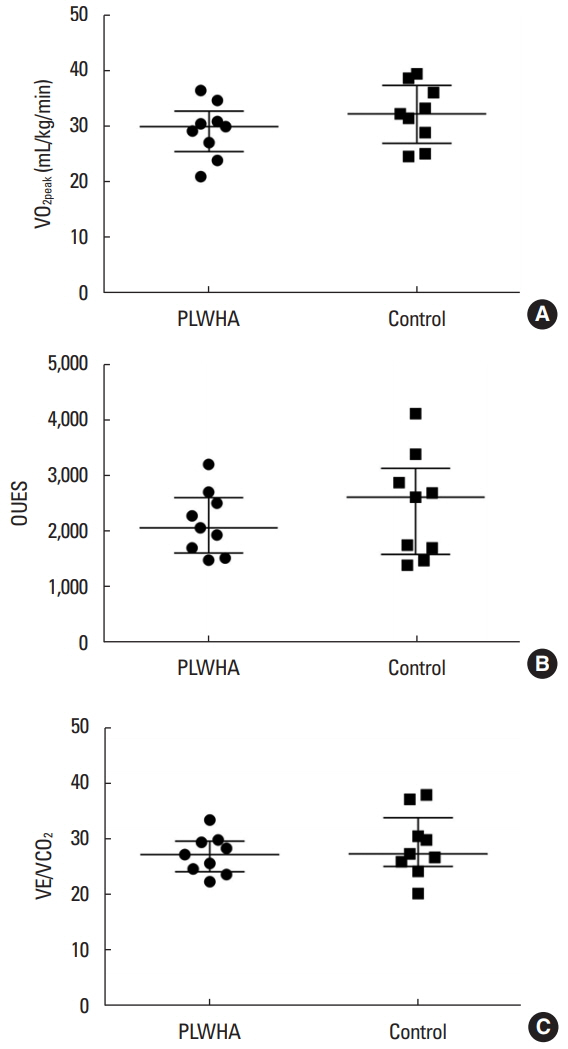
Both groups did not demonstrate significant differences in VO2peak, oxygen pulse, OUES, VE/VCO2 slope measured and predicted values (Table 2, Fig. 2), as well as GET and RCP measured and relative to VO2peak values. Likewise, HRR after the first and second minute immediately following CPX and T½ VO2 showed no differences between groups (Table 3).
There was a strong correlation between OUES and VO2peak in the PLWHA group (rs=0.70, P=0.04) and the control group (rs=0.78, P=0.02) (Fig. 3).
DISCUSSION
The results of this study show that PLWHA in HAART usage, physically inactive, but with well-controlled disease presented functional capacity and ventilatory efficiency similar to that observed in non-HIV/AIDS subjects. In addition, this study provides evidence that information obtained from CPX could be used as a basis for accurate prescription of aerobic exercise also in PLWHA. Besides that, due the similarity with the sedentary subjects, when CPX is unavailable, the aerobic assessment and prescription could be based on simple procedures used in healthy subjects, like estimated maximal HR, VO2peak/maximal and ventilatory thresholds.
Similar VO2peak values observed between groups, PLWHA and control, indicate the preservation of functional capacity and corroborate studies that assessed this outcome in PLWHA in the post-HAART era (De Lorenzo et al., 2013; Deresz et al., 2010). Oxygen consumption is obtained by the product of cardiac output and arteriovenous oxygen difference. In this way, the determinant variables of cardiac output (heart rate and systolic volume, here estimated by the oxygen pulse) (Guazzi et al., 2017), demonstrated no differences between the PLWHA and control group. These data justify, at least partially, the similarity between the results found in VO2peak. These results support the hypothesis of maintenance of functional capacity in PLWHA with well-controlled disease.
It would be important to note that the HAART, especially nucleoside reverse transcriptase inhibitors (NRTI) has been related to mitochondrial toxicity (Margolis et al., 2014) and reduced activity of oxidative enzymes, resulting in functional aerobic impairment (Cade et al., 2003). However, these side effects are more common in older NRTI drugs (didanosine, stavudine, and stavudine) than newer NRTI drugs (emtricitabine, lamivudine, and tenofovir) toxicity (Margolis et al., 2014). As the most of participants in this study were in newer NRTI drugs treatment is possible that have less propensity for causing mitochondrial toxicity and consequently, minor impact in functional capacity.
The OUES is a predictor of myocardial perfusion in coronary artery disease patients (Pinkstaff et al., 2010). In this study, OUES values showed no differences between groups, and when compared to the predicted values. This result could be explained by the equivalence found in the values of RCP, indirect marker of metabolic acidosis (Balady et al., 2010), and anthropometric parameters, body mass and body mass index, all variables that influence OUES determination (Defoor et al., 2006). Furthermore, in agreement with the literature (Baba et al., 1996), OUES may be used to estimate the cardiorespiratory functional reserve, because it shows a strong correlation with VO2peak. The main advantage of OUES in relation to VO2peak is that OUES may be obtained during the submaximal exercise test, which facilitates its measurement and use (Baba et al., 1996). In the present study, six participants were excluded because of not fulfilling the criteria for maximal physiologic effort (RER≥1.1) and therefore their functional capacity was not properly evaluated.
This circumstance could have been modified by the use of a variable obtained during the submaximal test, for example, OUES, supporting the use of this variable as an indicator of cardiorespiratory reserve (Baba et al., 1996).
The VE/VCO2 slope is predictors of cardiac-related mortality and hospitalization in heart failure patients (Arena et al., 2004). In this study no difference in VE/VCO2 slope measured and predicted values were observed between the groups. In heart failure patients (Arena et al., 2007), one of the possible causes of elevated VE/VCO2 slope is the decline of lung perfusion and thus, a reduction in CO2 exchange, as a result of decreased cardiac output which is a consequence of reduced cardiac capacity. The present study did not measure cardiac output and cardiac capacity, however, oxygen pulse and HRmax that are, respectively, indirect indicators of cardiac output and cardiac capacity, showed no difference between the groups, which explains, in part, the VE/VCO2 slope values within the normal range.
Heart rate recovery (Cole et al., 1999) and T½ VO2 (Cohen-Solal et al., 1995) values were within normal ranges. Both, HRR, and T½ VO2, have been considered predictors of mortality in healthy subjects (Cole et al., 1999) and patients with chronic heart failure (Cohen-Solal et al., 1995). Normal HRR response is suggestive of parasympathetic system integrity (Imai et al., 1994) and good cardiovascular health (Cole et al., 1999). In addition, T½ VO2 values suggest that muscle oxidative capacity is also preserved (Cohen-Solal et al., 1995). These results suggest that the integrity of the cardiovascular system is preserved in PLWHA with well-controlled disease, without compromising oxidative metabolism.
It has been described that the myocardial metabolism is normal in PLWHA with well-controlled disease and that cardiac metabolism is dependent on the metabolic complications present in the disease and not from the HIV infection (Cade et al., 2011). As most of the participants of previous study did not have metabolic abnormalities, it is possible that this explanation is also applicable in our sample. Similarly, the pulmonary abnormalities are more associated with smoking history and tuberculosis (Sampériz et al., 2014), disease severity (T CD4+ <100 cells/mm3) and high viral load, >75,000 copies/mL (Drummond et al., 2013) than to HIV infection per se (Drummond et al., 2013; Sampériz et al., 2014). In the present study, PLWHA had well-controlled clinical condition, no cases of tuberculosis treatment and there were no smokers, thus, normal lung function was expected.
Despite having normal levels of functional capacity and ventilatory efficiency, PLWHA should be encouraged to participate in exercise training programs, to gain additional benefits, such as cardiorespiratory fitness, strength, lean body mass, body composition (O’Brien et al., 2017) and metabolic disorders (Lindegaard et al., 2008). For better results, exercise training should follow the recommendations from the American College of Sports Medicine (Garber et al., 2011) for physical exercise prescription. These recommendations suggest that information obtained using CPX could be used in both the evaluation of functional capacity and for the precise prescription of exercise.
This study has limitations inherent to the sample size. More specific measures of body composition and lung function might reinforce the observed results. Moreover, generalization of the present results should be performed with caution because only subjects on HAART, with well-controlled clinical conditions and nonsmokers were evaluated, which can limit the possibility to extrapolate the results to a different evaluated sample.
The main results of this study indicate that functional capacity and ventilatory efficiency are preserved in PLWHA with well-controlled disease. These findings suggest that adequate treatment adherence and success in clinical management contribute to the integrity of cardiac, ventilatory and metabolic responses to physical exercise. Furthermore, CPX could be used to prescribe aerobic exercise and to evaluate functional capacity in PLWHA with well-controlled disease. It is necessary to highlight that the results from the present study do not exclude the necessity of the PLWHA in performing exercise training programs to enhance functional capacity and, consequently, quality of life.