Effects of proprioceptive neuromuscular facilitation and both sides up ball exercise on pain level, range of motion, muscle function after total knee arthroplasty
Article information

Abstract
Knee osteoarthritis (OA) is a degenerative joint disease caused tearing and progressive wear of articular cartilage, and total knee arthroplasty (TKA) is recommended to patients with OA. The purpose of this study was to investigate the effect of proprioceptive neuromuscular facilitation (PNF) and both sides up ball (BOSU) exercises on pain, range of motion (ROM), and muscle function in patients following TKA. Ten participants who have limitation of the knee joint from TKA were divided into two groups: the continuous passive motion (CPM)+PNF exercise group (n=5) and the CPM+BOUS exercise group (n=5). Exercise rehabilitation program consisted of PNF and BOSU exercises, and both exercises were performed twice a day for 2 weeks. To examine effect of exercise rehabilitation, visual analogue scale (VAS), sit and reach flexibility, knee ROM, and Timed Up and Go test (TUG) were measured before and after exercise intervention. A two-way repeated analysis of variance was used to confirm the main effect. If there was a significant interaction effect, an independent t-test between groups or a paired t-test between times was applied. VAS, sit and reach flexibility, knee ROM and TUG did not show interaction between the PNF and BOSU exercise groups, but all measured variables showed significant differences over time. Present findings provide information that PNF and BOSU exercise rehabilitation after TKA might be an important part of ensuring successful surgical outcomes as they have a positive impact on reducing pain, increasing ROM, improving muscle strength, and enhancing daily life movements.
INTRODUCTION
The knee joint is one of the largest and most complex joints in the human body and belongs to a synovial joint that connects the femur, tibia, and patella. The knee joint also is stabilized by surrounding skeletal muscles, tendons, and ligaments, but it is a joint with a high risk of injury in daily life or sports activities (Albtoush et al., 2018).
Knee osteoarthritis (OA) is a degenerative joint disease caused tearing and progressive wear of articular cartilage. Patients with OA have reduced lower limb strength and exercise performance due to pain and inflammation in the knee joint. Specifically, it has been reported that joint stiffness and deformation, and decreased proprioceptive function in OA patients decrease the patient’s balance ability, leading to a decline in quality of life (Knoop et al., 2012). To treat patients with OA, nonsurgical treatments such as drug therapy, physical therapy, exercise therapy are primarily applied. However, If the degree of joint damage is severe and extreme pain interferes with daily life, total knee arthroplasty (TKA) is recommended (Canovas and Dagneaux, 2018).
Patients who undergo a TKA often experience loss of mobility due to pain at surgical site (Canovas and Dagneaux, 2018). Mobility in patients following TKA is closely associated with range of motion (ROM) of the knee. A decrease in knee ROM not only reduces lower extremity muscle strength over time, but also induces joint stiffness (Zeni and Higginson, 2009).
Rehabilitation is one of the important steps after TKA to improve mobility deficit and knee ROM (Lenssen et al., 2008). Continuous passive motion (CPM) is mainly used to prevent joint contracture, increase ROM, and reduce pain in TKA patients. As an exercise rehabilitation approach to increase ROM, CPM mode using isokinetic device is the most widely used worldwide (Yang et al., 2019).
Proprioceptive function is a kinesthetic receptor located in muscles, tendons, and joints that primarily controls the sense of movement and posture (Prochazka, 2021). Proprioceptive neuromuscular facilitation (PNF) is a therapeutic technique that stimulates the proprioceptive sense through activating the response of neuromuscular mechanisms such as muscle spindles or tendon spindle organs (Sharman et al., 2006). Hindle et al. (2012) reported that PNF can regulate pain, muscle strength, ROM, and functional movement in people with the skeletal muscle weakness. Alaca et al. (2015) suggested that PNF technique is widely used in the treatment of not only patients with central nervous system disorders but also those with musculoskeletal issues including TKA patients.
Both sides up ball (BOSU) is an exercise equipment in the form of a hemispherical inflated ball that is flat on one side and convex on the other. Various BOSU exercises on an unstable platform can enhance balance and muscular strength at the same time (Behm and Colado, 2012). Squat exercises using BOSU have been shown to increase balance and improve muscle activity in the trunk muscles, glutes, and lower extremities (Saeterbakken et al., 2014). Furthermore, walking practice using BOSU during rehabilitation exercises for patellar pain syndrome has resulted in stable balance patterns and gait (Calatayud et al., 2017).
Previous studies on exercise rehabilitation for TKA patients have explored various PNF treatments, but research on BOSU exercise treatment remains limited. To promote mobility and physical activity in patients following TKA, a systematic exercise rehabilitation program is needed to reduce pain in the early stage of rehabilitation and improve lower extremity balance ability, ROM, muscle strength. Therefore, this study aimed to compare and analyze the effect of PNF and BOSU exercise on pain, ROM, and muscle function in TKA patients, and to present an exercise treatment program suitable for the early stage of rehabilitation.
MATERIALS AND METHODS
Participants
Participants in this study were only those who underwent 1–2 weeks after TKA surgery at Jeju Medical Center and expressed their intention to participate in this experiment. Ten elderly women participated and were randomly assigned two groups: the CPM+ PNF exercise group (n=5) and the CPM+BOUS exercise group (n=5) (Table 1). Before beginning the study, all participants had a detailed explanation of this study, and they submitted their written informed consent to the researchers. This research was conducted ethically according to international guidelines. This experiment obtained approval by the Ethics Committee of Jeju National University (2020-041).

Physical characteristics of the participants
Training program
The design of the exercise treatment program in this study was inspired by the work of Chow and Ng (2010), Lewek et al. (2001), and Verhagen et al. (2005) who reconstructed exercises rehabilitation program through tests and measurements related to the functional problems of TKA patients. To achieve the purpose of this study, exercise rehabilitation program was reorganized into PNF exercise and BOSU ball exercise to suit TKA patients. The overall exercise program is outlined in (Table 2).

Total of PNF and BOSU exercise program
PNF stretching program
The exercise rehabilitation program for the PNF-treated group consisted of 30 min of patient-tailed CPM (ARTROMOT-K1, ORMED GmbH, Freiburg, Germany) and 20 min of PNF. The hold-relax PNF technique was selected and applied twice a day for 2 weeks. And a combination of isotonic exercises and rhythmic inhibition were performed alternately once. In the first week, patient’s posture for the PNF treatment was lying down and sitting with legs spread. The hold-relax PNF technique, rhythmic stability, and isotonic exercises were performed for 10 sec each, followed by 10 sec of rest, for a total of 9 sets. In the second week, patient’s posture for the PNF treatment was lying down and sitting with knees bent. The treatment, rest times, and number of repetitions were the same as in week 1. The detailed exercise program contents of the PNF group are outlined in Table 3.
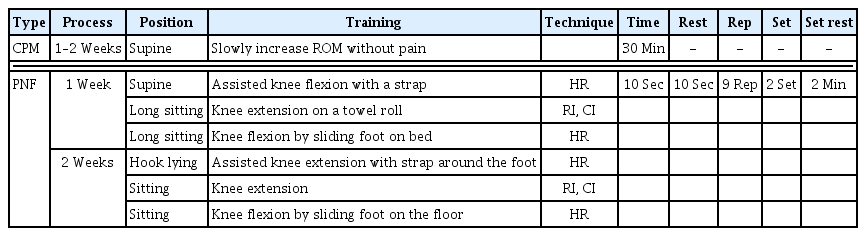
CPM and PNF exercise program
BOSU ball exercise program
The exercise rehabilitation program for the BOSU group was applied for a total of 2 weeks. In detail, CPM was tailored to the patient for 30 min, followed by 20 min of BOSU (Bosu Fitness, LLC, San Diego, CA, USA) exercises. In the first week, the BOSU exercise program consisted of isometric sitting, sitting and standing, and a static standing posture for 10 sec each, followed by a 10-sec rest, and a total of 9 sets were performed. The entire BOSU exercise treatment method was repeated twice. In the second week, the BOSU exercise program included dynamic standing, standing on one leg, and walking in place. The treatment duration, rest time, and number of repetitions were the same as in week 1. The detailed exercise program for the BOSU group is outlined in Table 4.

CPM and BOSU exercise program
Visual analogue scale
A visual analogue scale (VAS) is psychometric response scales to investigate a unidimensional measure of pain intensity, and it is widely used in clinical research to examine the intensity or frequency of pain (Paul-Dauphin et al., 1999). The VAS was a 10 cm horizontal or vertical line, and both ends were marked with no pain or the most severe pain. The subjects marked a point that matched the intensity of the pain they are currently feeling.
Sit and reach flexibility testing
To measure sit and reach flexibility, a body forward bending measuring device (SC633616, SKARO, Gunpo, Korea) was utilized. The subject sits on the box with the knee straight and the soles of both feet touching the vertical surface of the measuring device. They were then instructed to slowly bend their upper body forward and gradually push the measuring device with the middle fingers of both hands. The final position was noted at the point where the subject could no longer push further, and this value was recorded. Measurements were taken twice in total, and the maximum value (cm) was recorded.
Knee ROM testing
The knee ROM of the subject was measured by a physical therapist using universal and reliable goniometer (Baseline HiRes Plastic 360 Degree ISOM, Fabrication Enterprises, White Plains, NY, USA). The subjects lie on a bed in the supine position with their knee extended. And then the active ROM was measured by flexing the knee joint. To reduce the error between measurements, ROM test was repeated 3 times, and the average value was applied.
Muscle function testing
To evaluate lower limb muscle function, a Timed Up and Go test (TUG) was performed. This test, known as the stand-up and walk test, quickly measures walking and balance ability and is a highly reliable tool with inter- and intrarater reliability scores of r=0.98 to 0.99 (Podsiadlo and Richardson, 1991). For the measurement, the subject sits comfortably on a chair with armrests placed on a flat floor. Upon receiving a ‘start’ signal from the measurer, the subject stands up from the chair and walks as quickly as possible to a turnaround point 3 m away in the direction of the operated leg, then returns to sit down on the chair. The time required for one round-trip walk is recorded, with the test repeated a total of 2 times. The average time of these two attempts is then recorded.
Statistical analysis
PASW Statistics ver. 21.0 (SPSS Inc., Chicago, IL, USA) was used to determine the effect of PNF and BOSU exercise in patients with OA. To confirm the main effect, we used a two-way repeated analysis of variance. If there was a significant interaction effect, an independent t-test between groups or a paired t-test between times was applied. All values are expressed as mean±standard deviation. P<0.05 was considered significant.
RESULTS
PNF and BOSU exercises regulate pain sensitivity
To examine VAS scores for pain, we performed a subjective measure before and after applying PNF and BOSU exercises. As shown in Table 5, VAS score did not represent interaction effect (F=0.460, P<0.517) between groups and period, but there was a significant difference in the period within group (F=37.278, P<0.001). Both PNF (t=−5.041, P<0.007) and BOSU (t=4.025, P<0.016) exercises significantly decreased values for VAS in the posttest compared pretest.

The result for visual analogue scale (VAS)
PNF and BOSU exercises regulate flexibility
Changes of flexibility in TKA patients were investigated before and after applying exercise rehabilitation. As shown in Table 6, flexibility (sit and reach test) was not shown interaction effect (F= 1.087, P<0.328) between groups and period, however, there was a significant difference in the period within the group (F=14.579, P<0.005). PNF exercise (t=−4.009, P<0.016) significantly increased values for flexibility in the post test compared pretest.
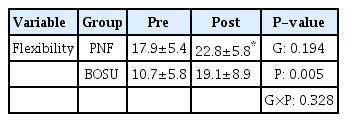
The result for flexibility
PNF and BOSU exercises regulate knee ROM
Changes of knee ROM before and after applying PNF and BOSU exercises were investigated. As shown in Table 7, knee ROM did not represent significant difference interaction effect (F=0.289, P<0.605) between groups and period, but there was a significant difference in the period within group (F=35.017, P<0.001). Both PNF (t=−3.478, P<0.025) and BOSU (t=−7.216, P<0.002) exercises significantly increased values for knee ROM in the post test compared pretest.
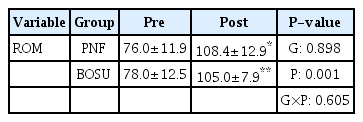
The result for rang of motion of the knee (ROM)
PNF and BOSU exercise regulate muscle function
Changes of TUG before and after applying PNF and BOSU exercises were investigated. As shown in Table 8, TUG was not shown interaction effect (F=0.008, P<0.932) and between groups and period, but there was a significant difference in the period within the group (F=19.143, P<0.002). Both PNF (t=2.895, P<0.044) and BOSU (t=3.364, P<0.028) exercises significantly decreased values for TUG in the post test compared pretest.
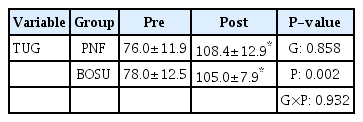
The result for Timed Up and Go test (TUG)
DISCUSSION
TKA is currently one of the most successful orthopedic surgical procedures performed when cartilage cells are damaged due to weakened ligaments and muscles in the knee joint. This surgery involves removing the severely worn joint surface and replacing it with an artificial joint (Carr et al., 2016). In the early stages postsurgery, almost all patients suffer from extreme pain, which tends to lessen over time. Pain in the knee joint generally reduces static and dynamic postural stability, balance ability, and increases the likelihood of falling due to reduced ROM of the knee (Puolakka et al., 2010). After TKA, it is crucial to apply a systematic and effective exercise rehabilitation program to improve pain, muscular strength, ROM of the knee (Dávila Castrodad et al., 2019). Our study examined changes in VAS scores according to the PNF and BOSU exercise programs and found significant reductions in pain level in both groups after rehabilitation program. Previous studies reported that early exercise rehabilitation including passive knee ROM exercises, patellofemoral joint mobilization, incision mobility and PNF decreased pain levels in patients with OA and TKA (Bade and Stevens-Lapsley, 2011; Song et al., 2020). This indicates a positive effect in patients who underwent TKA, supporting the results of this study.
ROM test has been often used in daily life and sports field to examine the joint mobility and performance capacity (Moreno-Pérez et al., 2020). In general, ROM is highly associated with increasing age and joint pain (Kennedy et al., 2013). In this study, flexibility (sit and reach) was improved in the PNF group posttest compared to pretest. Furthermore, both PNF and BOSU exercises significantly increased knee ROM after compared to before applying exercise rehabilitation program. The results suggest that the PNF and BOSU exercise programs improved flexibility by recovering knee stiffness and limited knee ROM in TKA patients. Immediately after surgery, TKA patients have complained of difficulty in undergoing exercise rehabilitation due to extreme pain, stiffness, and strong muscle contraction (MacDonald et al., 2000). Several previous studies reported that applying PNF to adults and athletes might improve ROM and flexibility function (Maicki et al., 2017; Smedes et al., 2016) as well as that exercise rehabilitation for TKA patients might stimulate proprioceptors within muscles and joints to restore ROM (Alaca et al., 2015; Yang et al., 2021). The application of various exercise rehabilitation is believed to have a positive effect on recovering ROM and flexibility function. Therefore, it is considered that TKR patients need diversity in their exercise rehabilitation programs, including both PNF and BOSU.
Increased quadriceps muscle strength is associated with functional stability of the knee joint, quality of life, and exercise performance. In addition, it has been reported that, in patients with ROM limitation such as TKA, the increase in quadriceps muscle strength at the initial stage of rehabilitation is one of the important factors determining the success of rehabilitation (Greene and Schurman, 2008; Paravlic et al., 2020). The results of these previous studies support the importance of PNF and BOSU in therapeutic strategy for developing the knee ROM.
Balance is the ability to maintain equilibrium with body’s center of gravity on various surface, and it is an essential physical capacity for static and dynamic stability of the body. To maintain functional balance, we must develop proprioception, integrated control of the central and peripheral nervous system, and vestibular sensory function (Lord and Fitzpatrick, 2001). TUG test, designed by Podsiadlo and Richardson (1991) has been used to evaluate walking ability, balance, and functional movement of older adults who had high risk of falling. Recently, it has also been applied to patients with stroke, Parkinson disease, and arthritis (Morris et al., 2001). In this study, the PNF and BOSU exercise programs resulted in faster TUG walking speeds. Previous studies by Saeterbakken et al. (2014) suggested that BOSU exercise improved lower extremity stability by enhancing muscle activation and balance ability. Also, when PNF exercise was administered to TKA patients, TUG times were significantly reduced (Blasco et al., 2017), and balance exercises notably improved mobility-related functions (Liao et al., 2015). The PNF and BOSU exercise programs are effective not only for TKA patients but also for the elderly and patients with stroke, Parkinson disease, and other conditions. Therefore, the PNF and BOSU exercise programs may be considered effective for improving walking ability in TKA patients.
Exercise rehabilitation after TKA is a crucial part of ensuring successful surgical outcomes, and this application have a positive impact on reducing pain, increasing ROM, improving muscle strength, and enhancing daily life movements. The number of TKA patients among elderly women is gradually increasing. Nevertheless, in this study, a small number of elderly participants provided consent for the exercise program. Due to the limited sample size, there are significant constraints in generalizing the results. Therefore, additional verification with larger samples will be necessary in the future.
ACKNOWLEDGMENTS
This research was supported by the 2022 scientific promotion program funded by Jeju National University.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.