Comparison of muscle activity during sit-to-stand movement at different chair heights between obese and normal-weight subjects
Article information

Abstract
The purpose of present study was to compare the tibialis anterior (TA), rectus femoris (RF), and erector spinae (ES) muscle activities at variety chair height during sit-to-stand (STS) on normal weight and obese subjects. Also, we compared the muscle activity difference between the normal weight and obese subjects. The study included 26 subjects (normal weight 13 and obese 13). Each subject performed STS at three chair heights (40 cm, 50 cm, 60 cm) and TA, RF, and ES muscle activities measured. According to the results of the measurement, muscle activation of TA showed significantly higher than RF and ES muscle activation during STS at all chair heights on obese subjects. The muscle activation of TA showed significantly higher than RF muscle activation during STS at all chair heights on normal weight subjects. The muscle activation of RF and ES showed significantly higher in normal weight subjects than obese subjects at 40 cm and 50 cm of chair heights. However, the TA muscle activation showed no significant difference between normal weight subjects and obese subjects. This study’s results suggested that obese subjects should practice the use of RF and ES muscles in a low-height chair during STS.
INTRODUCTION
Obesity is one of the commonest health-problem in industrialized countries (Sibella et al., 2003). As directly measuring body fat to diagnose obesity is complex and costly, obesity is generally categorized using body mass index (BMI), which is calculated as the weight (kg) divided by the square of the height (m2) (Kim and Park, 2017). BMI is indirect measurement, and does not perfect distinguish between body fat and lean body mass, however, BMI is strongly correlated with body fat levels (Kim, 2016). Adults in the Asia-Pacific Region are considered to be obese when their BMI is ≥25.0 kg/m2, overweight when their BMI is ≥23.0 kg/m2 and <25.0 kg/m2, and normal when their BMI is ≥18.5 kg/m2 and <23.0 kg/m2 (Kim and Park, 2017). Kim (2016) reported that BMI is not as accurate a predictor of body fat in the elderly as it is in younger and middle-aged adults. Previous studies were conducted on the association between various variable and obesity (Jang et al., 2016; Maffiuletti et al., 2007) and movement analysis (Galli et al., 2000) based on BMI in young adults.
Obesity can lead to comorbidities, the severity of which is proportional to excess body fat (Ryan et al., 2011). Obesity is related to a variety of musculoskeletal abnormalities in adults, which interferes with quality of life and functional capacity and increases healthcare costs (Anandacoomarasamy et al., 2008). Obesity can affect skeletal muscle function and thereby reduce movement of obese individuals (Teasdale et al., 2013). Several studies have described the negative effects of obesity such as systemic locomotor and musculoskeletal problems including weight bearing and postural balance changes (de Souza et al., 2005; Greve et al., 2007; Hills et al., 2001). Obesity alters kinematics during daily life activities such as sit-to-stand (STS) movement, contributing to the development of lower extremity joint injury, pain, and physical limitations (Runhaar et al., 2011). Previous studies reported that kinematic difference between normal and obese subjects during STS (Sibella et al., 2003), but it is still poor how muscles affect strategic components of STS in obese subjects. The strategies adopted by obese patients in STS movement can be analyzed to improve the design of rehabilitative treatment assessments (Galli et al., 2000).
STS movement is necessary for upright movement and other important daily activities (Bohannon et al., 2008). Thus, STS performance is fundamental for independence (Janssen et al., 2010). Within-subject factors such as knee extensor strength (Yoshioka et al., 2014), body mass (Huffman et al., 2015), initial foot position (Walaszek et al., 2017), and changes in seat height (Skowroński et al., 2009) contribute to STS performance. STS is an important functional task that may become difficult to execute in obese patients due to muscular weakness and other conditions (Galli et al., 2000).
STS motion requires optimal neuromuscular coordination and postural adjustments to control moment changes and prevent excessive energy generation or loss of balance (Papa and Cappozzo, 2000). The quadriceps is a primary motor muscle in STS, promoting knee extension and contributing to hip flexion and stability (Khemlani et al., 1999). The tibialis anterior (TA) is also important during the initial phases of the STS, to stabilize the foot on the ground (Lomaglio and Eng, 2005). The function of the erector spinae (ES) in STS movement is to provide early contraction and trunk extension, counteracting excessive trunk flexion (Fotoohabadi et al., 2010). Previous studies have reported the differential action of related muscles during STS motion when the initial seated posture changed (Goulart and Valls-Sole, 1999). Thus, the muscle activity of the lower limbs may change according to chair height during STS (Arborelius et al., 1992).
STS is an important functional task that may be more difficult for obese subjects to perform due to weight conditions, muscular weakness, and lower back pain. Recent studies have focused on kinetic and kinematic (Sibella et al., 2003) changes and lower limb muscle activity (Bollinger et al., 2019) during STS among obese subjects; however, few studies have explored the differences in muscle activity of the lower limb and trunk muscles according to chair height during STS motion among obese subjects. Therefore, in this study, we compared the electromyography (EMG) characteristics of lower limb muscle and trunk muscle at different chair heights during STS movement between obese and normal-weight subjects.
MATERIALS AND METHODS
Participants
A total of 26 participants (13 normal weight subjects and 13 obese subjects) were recruited in the study. The inclusion criteria were: (a) able to stand from an armless chair; (b) no muscular-skeletal pathologies; (c) no pain during movements; for normal weight group the inducing, criteria were BMI 18.5–22.9 kg/m2; for obese group the inducing, criteria were BMI>25 kg/m2. Ethics approval for this study was obtained from the Ethics Committee of the Kaya University (Kaya IRB-303). All participants were informed of the study’s purpose and content prior to the study.
Instrumentation
EMG activities of the three muscle on the lower limb and trunk during STS were recorded using surface Trigno wireless system (Delsys, Boston, MA, USA) and pairs of silver-silver chloride disposable electrodes with a diameter of 3 mm (EL 503, Biopac systems Inc., Goleta, CA, USA). The sampling rate was at 2,000 Hz. The EMG activity recording period of 5 secs. The threes in lower limb and trunk, were positioned over the muscle fibers of the rectus femoris (RF), TA, and the ES (Hermens et al., 2000). EMG data were normalized to reference voluntary contraction (RVC), the RVC testing was performed in subjects positioned in the quiet sitting. The data obtained from each trial were expressed as a percentage of the RVC.
Experimental procedure
Sit-to-stand maneuvers were performed from a chair without an arm rest. Chair heights were set at 40 cm, 50 cm, 60 cm (Yoshioka et al., 2014). STS began when a verbal signal from the tester. The movement strategy such as feet position, movement speed, and movement pattern was not restricted. This experiment was conducted in a random sampling manner. All subjects had to repeat the required motion for each height 3 times, taking a 2-min break between each repetition.
Statistical analysis
Data will analyze using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). The general characteristics were analyzed descriptive analysis. For identifying the normal distribution of data, the Kolmogorov–Smirnov test has been done before the statistical analysis. A one-way analysis of variance was used to compare the muscle activation according to the chair height during the STS on each group and Bonferroni method was used for post hoc tests. The comparison to muscle activation of normal weight and obese group on each chair height was analyzed using independent t-test. The statistical significance was set at P<0.05. The data were presented as the mean with standard deviation values.
RESULTS
General characteristics of the participants
The research participants included 26 male adults. Normal weight group average age was 19.7±1.25 years old, average height was 171.5±6.76 cm, average body weight was 59.3±6.76 kg, and average BMI was 20.3±1.07 kg/m2. Obese group average was 19.9±1.44 years old, average height was 173.2±10.4 cm, average body weight was 89.3±21.71 kg, and average BMI was 30.5± 4.4 kg/m2 (Table 1).
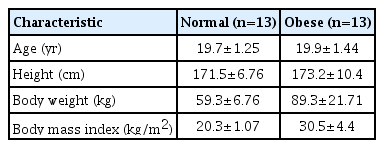
General characteristics of the participants (N=26)
The comparison of muscle activation according to chair height during STS on normal weight and obese subjects
There were significant differences between TA, RF, and ES muscle activation at all chair height on normal weight and obese subjects (P<0.05) (Table 2). The muscle activation of TA showed significantly higher than RF muscle activation during STS at all chair heights in both group (P<0.05) (Figs. 1, 2). The muscle activation of TA showed significantly higher than ES muscle activation during STS at all chair heights in obese subjects (P<0.01) (Fig. 1). By contrast, there was no significant difference between TA and ES muscle activation during STS at all chair heights in normal weight subjects (Fig. 2).
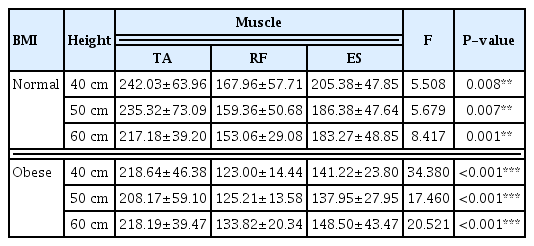
The comparison of muscle activation according to chair height during STS on normal weight and obese subjects
The comparison of muscle activity (%RVC) during sit-to-stand at different chair heights in obese subjects: tibialis anterior (TA), rectus femoris (RF), and erector spinae (ES). RVC, reference voluntary contraction.

The comparison of muscle activity (%RVC) during sit-to-stand at different chair heights in normal weight subjects: tibialis anterior (TA), rectus femoris (RF), and erector spinae (ES). RVC, reference voluntary contraction.
The comparison of muscle activation between normal weight and obese subjects during STS
The TA muscle activation was no significant difference between normal weight subjects and obese subjects at all chair heights (Table 3). The muscle activation of RF and ES showed significantly higher in normal weight subjects than obese subjects at 40 cm, 50 cm of chair heights (P<0.05) (Table 3).
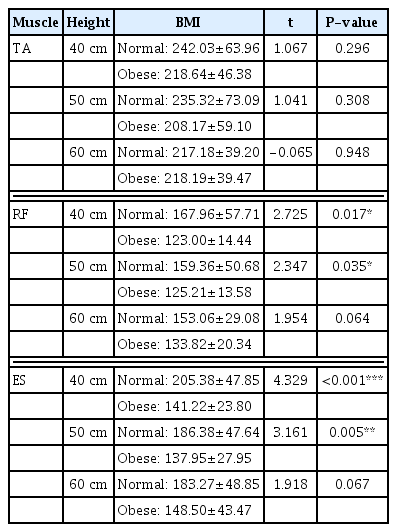
The comparison of muscle activation between normal weight and obese subjects during STS
DISCUSSION
Obesity can affect skeletal muscle function, reducing movement of obese peoples (Teasdale et al., 2013). Obese subject showed alters kinematics during STS movement compare to normal weight (Sibella et al., 2003), but it is few studies how muscles affect strategic components of STS in obese subjects. Therefore, this study investigated that difference in muscle activity during STS of obesity and normal weight.
This study observed higher muscle activity in the TA than the RF at all chair heights during STS movement in both groups. In a previous study, the TA showed the highest muscle activity during STS movement in a chair that was 43 cm tall among healthy subjects (Cuesta-Vargas and González-Sanchez, 2013); our findings are consistent with those findings. The TA is the first muscle to activate during STS, as an anticipatory postural activity that sets the center of gravity in the optimal position to stretch the more rostral joints without falling (Kasai and Kawai, 1994). This function could explain the high level of TA muscle involvement during STS performance. Our findings confirm the importance of the TA in stabilizing the foot during STS in obese subjects.
Present study showed that difference to between TA and ES muscle activity in all chair heights during STS performance in obese subjects but not in normal-weight subjects. STS is initiated by trunk flexion to provide horizontal momentum and shift the center of gravity forward; therefore, trunk flexion is the major kinematic strategy for improving STS performance (Walaszek et al., 2017). Normal-weight subjects rise from a chair by flexing the trunk forward and maintaining their feet in the initial position, whereas obese subjects limit forward trunk flexion and move their feet backwards from the initial position (Sibella et al., 2003). Obesity typically results in a more erect posture during STS (Galli et al., 2000; Sibella et al., 2003), suggesting that body mass may limit trunk flexion during this task. Body volume tends to alter kinematics during gait, independent of mass (Westlake et al., 2013); therefore, body volume may be a major driver of altered trunk kinematics during STS in obese subjects (Bollinger et al., 2019). It appears that obese subjects use the trunk extensor less than normal-weight subjects during STS, which may explain the differences in TA and ES muscle activity observed between obese and normal-weight subjects during STS in this study.
In the present study, RF muscle activity differed between obese and normal-weight subjects according to chair height during STS. At low seat height, higher load is imposed to the legs during STS movement (Ellis et al., 1984). Because seat height determines the load of STS movement (Janssen et al., 2002) and the thigh muscles contribute greatly to the achievement of this task (Corrigan et al., 2001), the subject’s dependence on thigh muscle activity is higher at low seat height. In addition, as seat height decreases, the knee flexion angle and moment will increase, leading to higher demand on the quadriceps to extend the knee as the body weight is lifted (Arborelius et al., 1992). Quadriceps muscle strength and power, relative to body mass, are lower in obese subjects than in nonobese subjects (Maffiuletti et al., 2007). By contrast, obese subjects have higher absolute knee extensor strength, but lower functional knee extensor strength, relative to body mass, for weight-bearing activities than normal-weight subjects (Tsiros et al., 2013). The amount and location of fat also appear to be associated with muscle function (Marsh et al., 2011). A previous study reported that obese subjects had twice as much intermuscular fat than normal-weight subjects, resulting in slower contraction velocity and reduced power generation (Choi et al., 2015). This finding is consistent with the hypothesis that muscle fat has a negative impact on muscles important for locomotion (Hilton et al., 2008). Total fat mass has been implicated as a predictor of functional decline, and fat infiltration into skeletal muscle has been found to be associated with lower muscle power (Sipila et al., 2004), as well as slower walking speed and chair rise times (Visser et al., 2002). Older adults with obesity have greater muscle mass and volume and higher absolute peak torque, but lower peak knee extensor torque normalized to thigh muscle volume, than normal-weight adults (Choi et al., 2015). The results of the present study also showed lower RF muscle activity in obese subjects due to a similar mechanism.
We found differences in ES muscle activity between obese and normal-weight subjects according to chair heights during STS. As previously discussed, obese subjects use the trunk extensor less than normal-weight subjects. Trunk flexion angular velocity increases with progressively lower seat height, indicating that this is an important adaptive strategy for STS motion (Schenkman et al., 1996). Obese subjects require greater trunk flexion velocity than their leaner counterparts at any given chair height (Bollinger et al., 2019). Therefore, compared to normal-weight subjects, obese subjects tend to complete STS with less trunk flexion (Galli et al., 2000; Sibella et al., 2003), thereby minimizing hip joint torque and lower back loading (Sibella et al., 2003). Our results suggest that the lower ES muscle activity observed in obese subjects is similarly caused by lower trunk flexion during STS. Therefore, it is thought that there was a difference compare the muscle activity on the normal weight subjects in the low chair height requiring more trunk flexion angle.
The present study had some limitations. Importantly, the muscle activity data were collected in all phases of STS movement. We also examined only a few lower limb and trunk muscles related to STS movement. Finally, we did not record kinematic data such as joint angle displacement throughout the experiment. Future studies should measure muscle activity in separate phases during STS, collect kinematic data, and include more muscle groups.
In summary, the results of this study demonstrate differences in muscle activity between normal and obese subjects during STS according to chair height. RF and ES muscle activity were lower in obese subjects than in normal-weight subjects at chair heights 40 cm and 50 cm. Previous study reported that obese subjects demonstrated a strategy characterized by limited trunk flexion to minimize the momentum on the lower back at the beginning of experimental session, whereas at the end of the session, they changed their rising strategy to increase trunk flexion (Galli et al., 2000). Therefore, obese subjects should practice the use of RF and ES muscles in a low-height chair during STS.
ACKNOWLEDGMENTS
This work was supported by the Kaya University.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.